Download
1 / 74
750 likes | 1.08k Views
Pelvic Fracture. Anatomy. 2 innominate 1sacrum Innominate bone ilium,ischium,pubis Join by strong ligament complex. Minor injury. Minor fall Stable vital sign Non-displaced Fx Fx not involve ring Treatment-bed rest. Minor injury. Major injury. High energy trauma

E N D
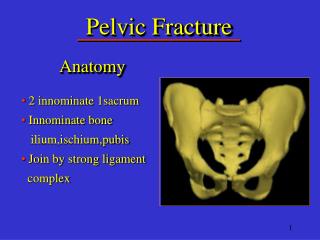
Pelvic Fracture Anatomy • 2 innominate 1sacrum • Innominate bone ilium,ischium,pubis • Join by strong ligament complex
Minor injury • Minor fall • Stable vital sign • Non-displaced Fx • Fx not involve ring • Treatment-bed rest
Major injury • High energy trauma • Unstable vital sign • High mortality,morbidity • Associated injury
Associated injury Rupture bladder Rupture urethra L-S plexus injury
Associated injury Hypovolemic shock Retroperitonium hematoma bleeding bony surface venous plexus bleeding vascular injury
SI joint widening Symphysis seperation Mechanism of injury AP compression (open book)
Fx ilium Lock symphysis Mechanism of injury Lateral compression(internal rotation)
SI dislocate Symphysis dislocate Mechanism of injury Vertical shear (Malgaigne Fx)
Major injury initial management • Recuscitation • Pelvic stabilization external fixator • Definite treatment pelvic sling ORIF
Fracture of proximal femur Surgical anatomy Vascular anatomy
Fracture neck of the femur • Intracapsular Fx • High rate of nonunion, avascular necrosis • 2 aged groups 1.Young adult high energy 2.Older with osteoporosis minor fall
Fracture neck of the femur • PE: • Limb slightly shortening • Pain at groin • Tenderness at midinguinal point Older patient ,minor injury Please X ray both hip AP ,lat crosstable
Treatment Young adult ,good bone quality Reduction and multiple pinning
Treatment Older with osteoporosis Hemiarthroplasty
Complication • Nonunion • Avascular necrosis • Venous thrombosis
Intertrochanteric Fracture • Fx line from greater to lesser trochanter • More common in woman menopause • Extracapsular fracture • Older with osteoporosis -minor fall
PE: • Limb shortening,external rotation • Swelling ,ecchymosis at hip • Tenderness at greater trochanter
Treatment Non operative traction 6 wks. high complications Pressure sore venous thrombosis infection
Operative treatment is preferable surgical risk, early ambulation
Subtrochanteric Fracture • Fx at level of lesser trochanter and a point 5 cm. Distally • thick cortical bone • high mechanic stress • high energy trauma
Treatment Operative treatment is preferable
Hip Dislocation • Posterior dislocation 80% most common • Anterior dislocation 5% • Central dislocation 15%
Posterior dislocation Blow to femur in adduction internal rotation of the hip Dashboard injury
Posterior dislocation PE: • hip flexion,internal rotate and adduct • ass.knee ligament injuries • assess sciatic nerve
X-ray • Head out of acetabulum • smaller femoral head • femur adduct, internal rotate(disappear lesser trochanter)
Treatment • Early diagnosis • prompt closed reduction • Allis’s maneuver • failed closed reduction-open reduction
Posterior dislocation Allis’s maneuver • Stabilized pelvis • longitudinal traction • 90 degree hip flexion • upward traction
Posterior dislocation Allis’s maneuver
Management after reduction • Test for stability • X-ray both hip AP evaluate joint space • Stable reduction skin traction- pain subside ambulation with crutches • Unstable reduction ORIF
Posterior dislocation Joint space widening Fragment entrap in joint
Anterior dislocation Blow to femur in abduction,external rotate of hip joint
Treatment • Early diagnosis • prompt closed reduction • Allis’s maneuver • failed closed reduction-open reduction
Anterior dislocation Reduction technique • General anesthesia • Traction along axis • Internal rotation • Lateral traction
Anterior dislocation Clinical manifestation X ray
Anterior dislocation Stabilized pelvis Internal rotation Traction along axis Lateral traction
Anterior dislocation Post reduction • X ray pelvis AP • Skin traction until pain subside(5-7 d) • Ambulation with crutches
Fracture shaft of the femur • High energy injury • Bleeding 1- 2.5 L. • Ass. femoral neck Fx. • Ass. hip dislocation
Physical examination • Deformity of thigh angulation shortening • PE.of hip and knee • Vascular assessmentdorsalis pedis a.posterior tibial a.
Management • Splinting - Thomas’s splint • Film femur include hip-knee detect neck Fx-dislocate hip • Temporary stabilization with proximal tibial traction
Management • Non-operative treatment Traction 6-8 wks. Femoral castbrace 10-12wks. • Operative treatment ORIF with plate-screw Intramedullary nailing
Transverse Fx midshaft femur ORIF with plate-screw
Comminuted Fx midshaft femur Intramedullary nail
Supracondylar fracture • Fx distal femoral metaphysis 9 cm. above joint line • Posterior displacement of the distal fragment • High rate of stiffed knee
Supracondylar Fx (extra-articular) Intercondylar Fx (intra-articular) T or Y Fx (combined) How to described Fx?
Treatment • Conservative Traction stiffed knee • Operative Early function Early knee motion
T Fracture of distal femur ORIF with plate and screw
Fracture of the patella • Largest sesamoid • Function -lever arm for knee extension -protect condyle
Avulsion(traction) Quads. pull up Knee flexion • Direct injury Mechanism of injury