Download
1 / 24
250 likes | 449 Views
Diabetes Management for the SPMI Population. Priscilla Swanson, RN, CCM, CHC, CPHQ Nancy Siegel, MPH, PA-C June 10, 2013 QHOC meeting. Background. Rates of diabetes are more than double those in the general population Newer antipsychotics may be inducing development of diabetes

E N D
Diabetes Management for the SPMI Population Priscilla Swanson, RN, CCM, CHC, CPHQ Nancy Siegel, MPH, PA-C June 10, 2013 QHOC meeting
Background • Rates of diabetes are more than double those in the general population • Newer antipsychotics may be inducing development of diabetes • Diabetes is harder to manage in the context of mental illness because it is largely a self-managed disease
Serious and Persistent Mental Illness (SPMI) Defined • An umbrella term that can include schizophrenia, bipolar illness, severe forms of major depression, obsessive-compulsive disorder, and panic disorders. • Any of these, if coupled with a persisting functional disability, is considered SPMI. Source: Kessler et al., 1994; U.S. Department of Health and Human Services, 1999
General Characteristics • Higher mortality rates • Many dependent upon public assistance • Many have two or more chronic illnesses with a higher prevalence of hypertension, diabetes, lung disease, alcohol, and substance abuse • Medical co-morbidities often go undiagnosed and untreated • Physical inactivity, which leads to higher obesity rates
General Characteristics (cont.) • Higher smoking rates (more than double general population) • Cognitive deficits, particularly with schizophrenia • Poor insight or awareness of illness • Affective response associated with the uncertainty and unpredictability of the disease
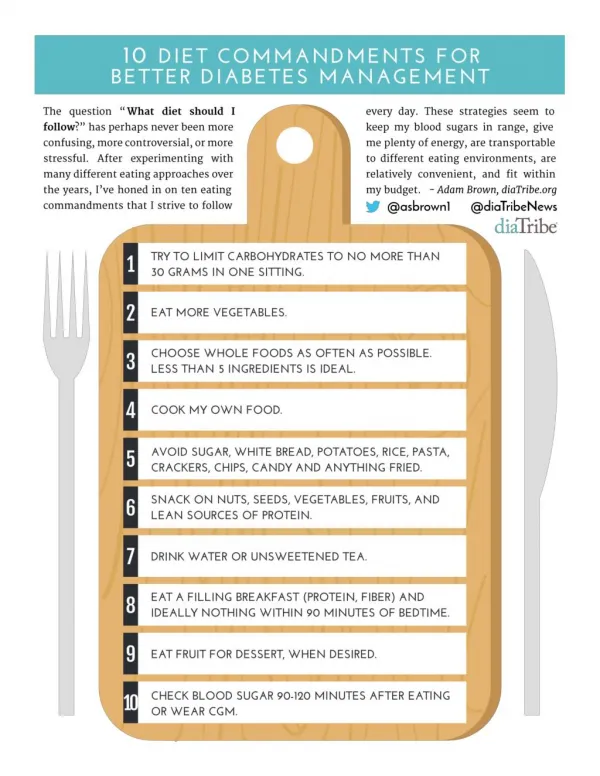
Basic Requirements for Diabetes Care with SPMI Population • Improve self-care ability • Obtain regular care • Stop smoking • Take prescribed medication
Clinical Practice Recommendations • Provide integrated care • Build a therapeutic alliance • Provide health information appropriately • Optimize client self-management
Clinical Practice Recommendations • Screen for diabetes • Treat pre-diabetes • Provide comprehensive diabetes care • Set appropriate goals for glycemic control • Provide case management
What Does “Integrated” Mean? “At the simplest level, integrated mental and physical health care occurs when mental health specialty and general medical care providers work together to address both the physical and mental health needs of their patients.” Source: Butler et al, 2008. Integration of Mental Health/Substance Abuse and Primary Care. AHRQ Publication No. 09-E003.
Evolving Models of Integration • Improved collaboration • Medically provided behavioral health care • Co-location • Disease management • Reverse co-location
Evolving Models of Integration (cont.) • Unified primary care and behavioral health • Primary care behavioral health • Collaborative system of care Source: Collins et al, 2010. Evolving Models of Behavioral Health Integration in Primary Care. Milbank Memorial Fund.
Providing Integrated Care • Medical services and behavioral health services located either in the same facility or in separate locations • One treatment plan with behavioral and medical elements • Typically a team working together to deliver care, using prearranged protocol
Providing Integrated Care (cont.) • Teams composed of a physician and one of more of following: • Physician assistant, nurse practitioner, nurse, case manager, family advocate, behavioral health therapist • Use of a database to track the care of patients who are screened into behavioral health services.
Insights on Integrated Care • “Make sure staff at all levels have bought into the model.” • “I recommend both parties participating, as we did, in quarterly problem-solving meetings to share each other’s dirty laundry–and mutually clean it.” • “The single biggest stumbling block was that we had no training period before services were to begin.” Source: Partners in Health: Mental Health, Primary Care and Substance Use Interagency Collaboration Tool Kit
More Insights • “It’s vital as you begin collaborations to have up-front discussions about important issues.” • “Training about the ins and outs of each other’s systems is absolutely necessary.” • “The building blocks are all about relationships and putting in the time needed to develop them–and the willingness to take risks and create innovations.”
Build a Therapeutic Alliance • Where possible, assign clients to one primary provider to build and maintain trust • Good relationships with health professionals are factors in patient success in complying with health recommendations
Provide Health Information Appropriately • Treatment may be more effective in an individual or family context, not group • “Errorless learning” approach • Interactive interventions that provide support, information, and management strategies for enrollees and families
Optimize Self-Management • Self-management ability changes depending on the status of the mental illness and current stressors • Use ongoing individual assessment • Care plan should be made and agreed upon collaboratively • Use client-centered methods to improve adherence in diabetes care
Screen for Diabetes • Ask about symptoms of diabetes routinely during health care visits • Perform diagnostic testing when symptoms are present • Screen for diabetes prior to starting antipsychotics. • Screen every 2-3 months during first year • Treat pre-diabetes
Case Management • Diabetes care is complex, requiring ongoing patient education and regular visits for health care and specialty referrals • Enhanced one-on-one support is needed to help resolve issues quickly and to ensure appointments are made/kept
Are You Ready to Select an Intervention? • Identify an appropriate intervention for the enrollees in your CCO • At minimum you will need to consider: • An increase in educational efforts • A change in policies/procedures • Potentially targeting additional resources • The culture shift and how to initiate mindful planning
Questions for Discussion • How you are integrating physical and behavioral services? • What steps have you taken to bridge the cultural differences between physical and behavioral health? • What intervention are you considering?
Resources • Integrated Behavioral Health Project. Partners in Health: Mental Health, Primary Care and Substance Use Interagency Collaboration Tool Kit. 2nd edition, 2013. http://www.ibhp.org/IBHP_Interagency_Collaboration_Tool_Kit_2013.pdf
Resources • Collins, et al, 2010. Evolving Models of Behavioral Health Integration in Primary Care. Milbank Memorial Fund. • McDevitt, J., 2002. Clinical Practice Recommendations: Evidence-Based Guidelines for Integrated Care. The Nursing Institute, College of Nursing, University of Illinois at Chicago.