The Endocrine System
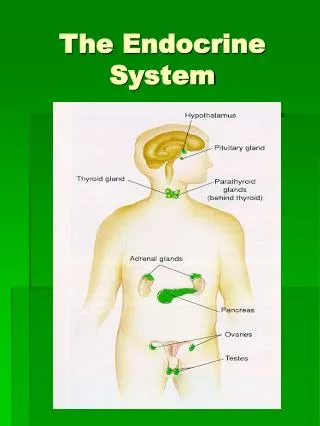
The endocrine system is a communication system in the body. It uses the blood circulation to transport hormones (in the blood plasma) around the body. . Endocrine Glands secrete hormones directly into the blood. They have no ducts. .

The Endocrine System
E N D
Presentation Transcript
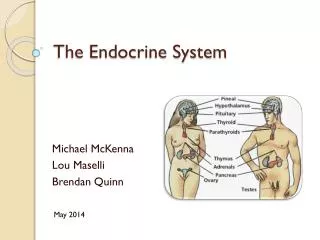
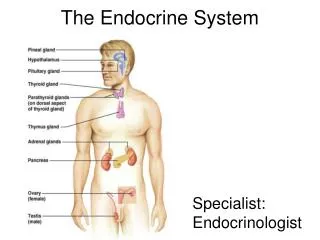
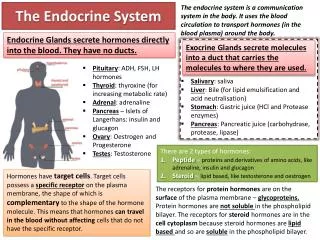
The endocrine system is a communication system in the body. It uses the blood circulation to transport hormones (in the blood plasma) around the body. Endocrine Glands secrete hormones directly into the blood. They have no ducts. Exocrine Glands secrete molecules into a duct that carries the molecules to where they are used. • Pituitary: ADH, FSH, LH hormones • Thyroid: thyroxine (for increasing metabolic rate) • Adrenal: adrenaline • Pancreas – Islets of Langerhans: insulin and glucagon • Ovary: Oestrogen and Progesterone • Testes: Testosterone The Endocrine System • Salivary: saliva • Liver: Bile (for lipid emulsification and acid neutralisation) • Stomach: Gastric juice (HCl and Protease enzymes) • Pancreas: Pancreatic juice (carbohydrase, protease, lipase) • There are 2 types of hormones: • Peptide – proteins and derivatives of amino acids, like adrenaline, insulin and glucagon • Steroid – lipid based, like testosterone and oestrogen Hormones have target cells. Target cells possess a specific receptor on the plasma membrane, the shape of which is complementary to the shape of the hormone molecule. This means that hormones can travel in the blood without affecting cells that do not have the specific receptor. The receptors for protein hormones are on the surface of the plasma membrane – glycoproteins. Protein hormones are not soluble in the phospholipid bilayer. The receptors for steroid hormones are in the cell cytoplasm because steroid hormones are lipid based and so are soluble in the phospholipid bilayer.
Adrenaline is synthesised from amino acids and is not soluble in lipids. Its target cells have receptors in their plasma membranes, to which adrenaline binds. Adrenaline 4. The adenylcyclase enzyme is activated. 1. Adrenaline attaches to specific complementary receptor on the outside of the plasma membrane. Receptor Adenyl Cyclase 2. Binding of adrenaline with its receptor alters the shape of the receptor, causing it to interact with another protein in the membrane called a G-Protein. ATP 3. The G protein splits, and one part of it combines with the inactive enzyme adenylcyclase. 5. Adenylcyclaseconverts ATP to cAMP. The cAMP can go on to activate other enzymes in the cell. G protein cAMP The first messenger is the hormone which binds to the receptor of the target cell. Here, it is adrenaline. The second messenger is the molecule activated inside of the target cell which can activate other enzymes. Here, cAMP is the second messenger.
Adrenaline and Adrenal Glands Adrenal Medulla – centre of gland Synthesises and releases adrenaline 1. Relaxes smooth muscle in bronchioles, bronchioles dilate, increase in breathing rate: blood is more fully oxygenated so that more oxygen is transported to muscles. Adrenal Cortex – edges of gland Uses cholesterol to produce steroid hormones 2. Increases stroke volume and heart rate: increases cardiac output to pump more blood per minute around the body carrying more oxygen and glucose to muscles for respiration. 4. Liver cells stimulated to convert glycogen to glucose in glycogenolysis: more glucose is supplied to muscles which can be used to make more ATP for contraction. 3. Vasoconstriction of blood vessels supplying digestive system and other organs, vasodilation of vessels to brain and skeletal muscles: this diverts blood flow to where it’s needed most – more blood carrying oxygen and glucose reaches muscles and brain. • Mineralocorticoids help to control the concentrations of sodium and potassium in the blood • Glucocoticoids control metabolism of carbohydrates and proteins in the liver. 5. Dilates pupils and increases mental awareness: helps to identify and respond to danger.
The pancreas has both endocrine and exocrine function. The Pancreas The exocrine function is the release of enzymes. The endocrine function is the secretion of hormones – glucagon and insulin. Pancreatic juice also contains sodium hydrogen carbonate. This neutralises the acidic chyme entering the duodenum from the stomach, because enzymes there have an optimal pH of neutral or just above. • Acinar cells secrete pancreatic juice into the duodenum of the small intestine. The pancreatic juice contains 3 types of enzymes: • Amylose – breaks down starch into maltose • Trypsinogen – breaks down proteins into shorter polypeptides • Lipase – breaks down lipids onto glycerol and fatty acids. The α cells and β cells are specialised to manufacture and secrete hormones. They have lots of rough endoplasmic reticulum for protein synthesis; lots of golgi, for the modification and packaging of insulin and glucagon; lots of vesicles for secretion of hormones by exocytosis. The islets of Langerhans are small patches of tissue in the pancreas containing α cells that secrete glucagon and β cells that secrete insulin.
Islets of Langerhans: Insulin and Glucagon α cells and β cells– endocrine – secreting glucagon and insulin Insulin decreases blood glucose • Insulin increases the ability of muscle cells and adipose tissue to absorb glucose from the blood. Muscle cells have glucose transporters called GLUT4, which are normally kept in the cytoplasm. When insulin is detected, transporters are moved into the plasma membrane where they form channels allowing glucose to enter. • Increased rate of conversion of glucose to glycogen: insulin activates glucokinase enzyme, which phosphorylates glucose. It also activates glycogen synthase which causes α 1-4 glycosidic bonds to form between glucose molecules, producing glycogen. Acinar cells – exocrine – releasing pancreatic juice into the pancreatic duct. Glucagon increases blood glucose • Increases the rate of conversion of glycogen to glucose – glycogenolysis: glucagon binding to receptors on the liver plasma membrane causes the activation of enzymes that catalyse the hydrolysis of glycogen to glucose. • Increase rate of production of glucose from other substances in the cell – gluconeogenesis: glucose is made from amino acids or lipids. Insulin targets liver and muscle cells. Glucagon targets liver cells only. The secretion of insulin and glucagon work as part of a negative feedback mechanism to keep blood glucose levels fairly constant – oscillating around the normal level of 90mg/100cm3 of blood.
Regulating Blood Glucose: Homeostasis • Blood Glucose Too High: • Detected by β cells. • β cells secrete insulin; α cells stop secreting glucagon • Insulin targets muscle and liver cells • Increased absorption of glucose; increased respiration of glucose; increased conversion of glucose to glycogen • Blood glucose level decreases • Blood Glucose Too Low: • Detected by α cells • α cells secrete glucagon; β cells stop secreting insulin • Glucagon targets liver cells only • Increased conversion of glycogen to glucose (glycogenolysis); increase production of glucose from other compounds (gluconeogenesis); decreased respiration of glucose (increased respiration of fatty acids) • Blood glucose level increases
βCells : Insulin Secretion 1. Cell membranes of β cells contain potassium and calcium ion channels. 2. Normally, the K+ channels are open, allowing K+ ions to pass through the membrane freely. They usually diffuse out of the cell, making the inside of the cell more negative, around -70mV. 3. When the glucose levels around the β cell are high, more glucose diffuses into the cell through transporter proteins. 5. The K+ channels are sensitive to the amount of ATP in the cell: an increase in ATP concentration causes them to close. 4. As the glucose enters the cell, it is phosphorylated by glucokinase and then metabolised to form ATP. 6. As K+ cannot diffuse out, the cell potential increases – becoming less negative. 7. The change in potential difference causes Ca2+ channels to open. The calcium ions cause vesicles containing insulin to move to the plasma membrane and fuse with it, releasing insulin by exocytosis.
Diabetes is a disease in which blood glucose concentrations cannot be controlled effectively. Diabetes Mellitus Type II diabetes is non-insulin dependent diabetes. A person with type II diabetes can still produce insulin, but the liver and other target organs do not respond to it adequately. There are several risk factors for type II diabetes: obesity; a sedentary lifestyle; family history; a diet high in sugars; being of Asian or Afro-Caribbean origin. Type I diabetes is insulin-dependent diabetes. It usually starts in childhood. It is thought to be the result of an autoimmune response in which the body’s own immune system attacks the β cells and destroys them. The pancreas is unable to secrete enough insulin, resulting in blood glucose levels soaring after a carbohydrate-containing meal. • Diabetes can lead to: • Hyperglycaemia – very high concentrations of blood glucose after a meal rich in carbohydrates • Hypoglycaemia – very low concentrations of blood glucose following fasting or exercise. • Treating Diabetes • Type II diabetes can usually be treated by careful monitoring and control of diet. Care is taken to match carbohydrate intake and use. Eventually, this may be supplemented by insulin injections or other drugs which slow down the absorption of glucose from the digestive system. • Type I diabetes is treated using insulin injections. The blood glucose concentration must be monitored and the correct dose of insulin administered to keep glucose levels fairly constant.
Sources of Insulin: GM Insulin • Made by genetically modified E. Coli bacteria • It is an exact copy of human insulin, so it is faster acting and more effective • There is less chance of developing a tolerance to the insulin • Less chance of rejection due to immune response • Lower risk of infection • Cheaper to manufacture insulin than to extract it from animals • Manufacturing process more adaptable to demand • People less likely to have moral objections to using insulin made from bacteria than insulin extracted from animals. Treating Diabetes with Stem Cells? Stem cells obtained from blastocysts are totipotent, meaning that they are able to differentiate into any kind of specialist cell. In theory, transplanting embryonic stem cells into someone’s pancreas can provide them with new β cells. • Stem cells are undifferentiated cells that are able to divide and form specialised cells. • It is hoped that in the future, it will be possible to transplant stem cells into a pancreas that has no functioning β cells, and they will form new β cells that can produce insulin.
Control of Heart Rate The heart muscle is myogenic – it can initiate its own contractions. The heart contains its own pacemaker cells – called the Sino Atrial Node. The SAN is a region of tissue that initiates an action potential that travels as a wave of excitation over the atria walls, through the AVN and down the Purkyne fibres to the ventricles, causing them to contract. • In order to supply more oxygen: • Heart rate increases (more beats per minute) • Stroke Volume increases – larger volume of blood pumped per beat • Stronger muscle contraction The heart is supplied with nerves from the medulla oblongata of the brain. These nerves connect to the SAN and affect the frequency of the waves of excitation. Motor Innervation: Action potentials sent down the accelerator nerve (a sympathetic nerve) increase heart rate. Action potentials sent down the vagus nerve (a parasympathetic nerve) decrease the heart rate. Blood pressure is monitored by baroreceptors (stretch receptors)in the walls of the carotid sinus. If the blood pressure rises too high, the stretch receptors send signals to the cardiovascular centre, which responds by reducing heart rate. Medulla Oblongata Sensory Innervation – Responding to internal stimuli: the heart must be able to respond to changes in blood pressure or carbon dioxide concentration. Movement of the limbs is detected by baroreceptors (stretch receptors) in the muscles. These send impulses to the cardiovascular centre informing it that extra oxygen may soon be needed. This tends to increase heart rate. Chemoreceptors in the medulla oblongata, carotid arteries and aorta monitor carbon dioxide levels and blood pH. These chemoreceptors send impulses to the cardiovascular centre which increases the heart rate.