Download
1 / 43
430 likes | 600 Views
MASSIVE ANTERIOR CHEST WALL ABSCESS COMPLICATING IMPACTED MANDIBULAR THIRD MOLAR INFECTION. AKINBADE A.O, F.J OWOTADE. INTRODUCTION.

E N D
MASSIVE ANTERIOR CHEST WALL ABSCESS COMPLICATING IMPACTED MANDIBULAR THIRD MOLAR INFECTION AKINBADE A.O, F.J OWOTADE
INTRODUCTION • Odontogenic infection occasionally spread and descend through the deep fascial planes of the neck leading to life-threatening sequelae such as mediastinitis and pleuropulmonary suppuration. • Chest wall abscess is an uncommon condition. • When it occurs, it is usually caused by Mycobacterium tuberculosis or secondary to open trauma or thoracic wall surgery.
It can evolve from simple soft tissue infection, osteomyelitis of the ribs, infection of the sternoclavicular joint or costochondral junction. • However, anterior chest wall abscess from odontogenic infection is extremely rare. • Fascial spaces of the neck communicate in a complicated and unpredictable manner.
Involvement of any of lateral pharygeal, retropharygeal and pretracheal spaces can be severe and associated with longer hospital stay. • The purpose of this paper is to report a rare case of massive anterior chest wall abscess arising as a complication of odontogenic infection in relation to an impacted third mandibular molar.
CASE REPORT • A 40 year old woman presented with: • One month history of toothache from the left side of the lower jaw. • Painful swelling involving the jaw and neck on both sides • Associated purulent discharge from the left mandibular third molar and the chin two weeks prior to presentation
She presented in a private clinic few days before coming to us where submental incision was done and was said to have been transfused three units of blood. • There was moderate difficulty in breathing, mastication and swallowing as well as fever malaise and generalized body weakness. • No history of trauma to the jaws nor previous history of jaw swelling.
She developed a big painful swelling on the upper right side of chest and shoulder region a week before presentation which became ulcerated and started producing copious purulent bloody discharge. • Medical history was not significant and no history suggestive of immunosupression nor bleeding disorders. • There was chest pain, orthopnea, cough not productive of sputum and dysphagia. • Patient is a petty trader and married to a farmer.
CLINICAL EXAMINATION` • On clinical examination: • patient was a toxic-looking middle-age woman in respiratory distress, conscious and alert. • She was markedly pale, acyanosed and anicteric, no pedal edema.
Blood pressure was 80/30mmHg, respiratory rate 40 cycles /min, pulse rate 120beats/min, temperature 38.6 C. • chest movement was symmetrical, the right chest and was dull to percussion and breath sound was reduced on the right hemithorax. • The abdomen was flat otherwise no other abnormal findings.
Examination of the head and neck revealed mild diffused left submandibular swelling ,a spherically shaped incision in the mental region of about 3mm in diameter with no active discharge. • Moderate swelling on the right side of the neck which extended to involve the right supraclavicular region.
There was a massive spherically shaped tender swelling on the upper part of the right anterior chest wall extending posteriorly to the scapular region • Measured about 20cm in widest diameter. The swelling is largely fluctuant with a brawny hard consistency in the periphery
There was an incisional wound on the central region of the swelling actively discharging copious bloody exudates. No areas of necrosis but the skin overlying the swelling is markedly erythematous and warm to touch
There was no bony discontinuity of the facial skeleton nor significant limitation of mandibular movement. • The left submandibular lymph node was palpaple and slightly tender.
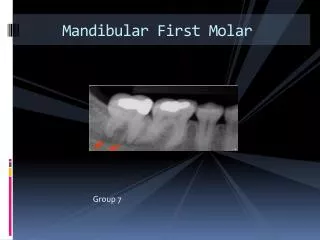
CLINICAL EXAMINATION • Intra-oral examination revealed poor oral hygiene with presence of ropy saliva and pus discharge from the gingival crevice in relation to the left mandibular third molar which was partially erupted, carious and slightly mobile. Other teeth are otherwise intact.
INVESTIGATION • The following findings were made from heamatological and biochemical investigations of the patient at presentation, PCV-13%, creatinine- 122mmol/l,bicarbonate-24mmol/l, potassium – 3.2mmol/l, Sodium-132mmol/l, Urea- 4.9 mmol/l, random blood glucose-7.1 mmol/l. Screening for HIV-1 and 2 was negative.
DIAGNOSIS • A diagnosis of massive anterior chest wall abscess secondary to spreading odontogenic infection, complicated by severe anaemia and septiceamia was made.
RADIOLOGICAL INVESTIGATION • Radiological investigation of the jaws, neck and chest revealed: • Grossly normal mandible • Mesioangularly Impacted and grossly carious lower left third molar with apical luscency • loss of normal cervical lordosis and patchy opacities at C4-C6, opacity of the upper right zone of the chest, cardiophrenic and costophrenic angles were bilaterally intact
INVESTIGATION • Patient could not afford the cost of other investigations like blood culture, clotting profile or CT.
TREATMENT • Intravenous infusion of 0.9% normal sline • IV ceftriaxone 1g daily • IV metronidazole 500mg 8hrly • IV genticin 80mg 8hrly • Urgent wound exploration, incision and drainage under GA was planned but patient could not afford the cost.
Daily dressing of the chest wound was done with EUSOL was always associated with copious bloody discharge. • Antimicrobial therapy was interrupted and blood transfusion was delayed due to patient’s financial situation.
Patient surprisingly improved overtime as chest wound began to granulate well at the 4th week of admission. • Discharged to outpatient clinic at the 5th week. • She absconded and resurfaced 8 months after discharge when the offending impacted molar was extracted.
DISCUSSION • Chest wall abscess is an uncommon condition. • When it occurs it is usually caused by Mycobacterium tuberculosis or secondary to open trauma or thoracic wall surgery.
Chest wall abscess caused by Mycobacterium tuberculosis usually run an indolent low grade course. • Unlike this case it appears as a slow growing mass with no associated symptoms- cold abscess. • Sakran and Bishrat in a recent review of chest wall abscesses found no case that was of odontogenic origin.
Yuvaraj and Krishnan reported the only case of anterior chest wall abscess arising from odontogenic infection in the literature. • Their case was not as massive and fulminant as this present one.
Mandibular third molar is the most frequently associated with severe fascial space infection. • Because their roots are usually inferior to the mylohyoid line. • Pericoronal or periapical infections from this tooth like the present case spread directly into the connective tissue of the submandibular space.
This rapidly spread to the contralateral submandibular space through the adjoining sublingual spaces. • At this point, the infection can directly spread inferiorly or posteriorly on either side to involve the lateral pharygeal space.
The lateral pharygeal space occupy a pivotal position in the neck as it communicaes with all the major fascial spaces. • From this point rarely, as in the case of this patient, the infection follows the platysma and spread between the clavicle and first rib to the anterior chest wall.
What determines whether an infection in the deep cervical fascia will spread to the mediastinum or the anterior chest wall is the density and strength of the pleurovertebral and costopleural ligaments. • If they are strong enough infection may be directed superficially to the anterior chest wall thereby preventing an extension into the mediastinum.
This case is peculiar in that the abscess collected on the contralateral chest wall. • Positioning of the head on the right side when patient lies in other to avoid stimulating pain from the offending tooth on the left side may favour gravitation and collection more on the right side.
This case demonstrate the poor health seeking behaviour of people of low socioeconomic status in the Nigerian population which was reported as a risk factor for severe odontogenic infection.
Poor oral hygiene and abuse of antibiotics which has led to emergence of community acquired antibiotic resistance may have contributed to the unusual course of the infection. • The absence of other co-morbidities and immunosupression may have aided the eventual recovery of the patient.
The absence of severe life-threatening embarrasment in this patient could be explained by the fact that the mediastinum was not involved. • This also reduced the risk of mortality in the patient unlike mediastinitis.
Immediate and aggressive surgical drainage of this abscess is critical in this case. • Effective antibiotic and supportive therapy as well as the removal of the source of infection as early as possible are all determinants of the outcome of this infection.
CONCLUSION • Anterior chest wall abscess can be caused by spreading odontogenic infection. • This abscess may run a aggressive course compared to that caused by the ones due to other Mycobacteria spp which is usually indolent.
All Clinicians should be aware of the possibility and manner of this unusual presentation. • Prompt and definitive surgical intervention is needed in order to reduce morbidity and prevent mortality.
REFRENCES • Chow WA, Rosen SM, Brady FA. Orofacialodontogenic infection. Ann Intern Med 88:392,1978. • V. Yuvaraj,Balasubramanium Krishnan. Anterior chest wall abscess: an unusual complication of an odontogenic infection. Oral MaxillofacSurg 2010;14:239-241 • Dubrul EL. Sicher and Dubrul’s Oral Anatomy, 8thedn. IshiyakuEuroAmerica, St Louis, Missouri. Pp 299-311 • WaheebSakran, NaielBisharat. Primary chest wall abscess caused by Escherichia coli constochodritis. Am J Med Sci 2011;342(3):244-246.
REFERENCES • Lo Cicero J. Infections of the chest wall. In shield T, editor. General thoracic surgery. Philadelphia(PA): Linppincott Williams Wilkins; 2005 p 682-8 • Flynn TR, Shanti RB, Haye C. Severe odontogenic infections part 1 prospective report. J Oral MaxillofacSurg 2006:64:1104-13 • Akinbami B.O, Akadiri O, Gbujie DC. Spread of odontogenic infections in Port Harcourt, Nigeria. J Oral MaxillofacSurg 2010;68:2472-2477
Topazian RG(2002). Odotogenic infections and deep fascial space infections of dental origin. In Topazian RG, Goldberg MH, Hupp JR(eds). Oral and Maxillofacial infections. 4thedn. WB Saunders , Philadelphia pp158-18 • Agarwal AK, Serthi D, Mrig S, Chopra S. Role of Socioeconomic factors in deep neck abscess: a prospective study of 120 patients. Br J Oral MaxillofacSurg 2007;45(7):553-555. • Viera F, Allen SM, Stocks RM, Thompson JW. Deep neck infection. OtolaryngolClin North Am 2008;41(3):459-483.