Download
1 / 52
540 likes | 855 Views
CONTROL OF EXTRACELLULAR FLUID VOLUME AND REGULATION OF RENAL NaCL EXCRETION. The typical diet contains approximately 140 mEq /day of Na + (8 g of NaCl ), and thus daily excretion of Na + in urine is also about 140 mEq /day.

E N D
CONTROL OF EXTRACELLULAR FLUID VOLUME AND REGULATION OF RENAL NaCL EXCRETION
The typical diet contains approximately 140 mEq/day of Na+ (8 g of NaCl), and thus daily excretion of Na+ in urine is also about 140 mEq/day. • However, the kidneys can vary the excretion of Na+ over a wide range. Excretion rates as low as 10 mEq/day can be attained when individuals are placed on a low-salt diet. • Conversely, the kidneys can increase their excretion rate to more than 1000 mEq/day when challenged by the ingestion of a high-salt diet. These changes in excretion of Na+ can occur with only modest changes in ECF volume and the Na+ content of the body.
Volume sensing system(Volume and Na+ Sensors ) I. Vascular volume sensor A. Low pressure 1. Cardiac atria 2. Pulmonary vasculature B. High pressure 1. Carotid sinus 2. Aortic arch 3. Juxtaglomerular apparatus of the kidney II. Central nervous system Na sensor (hypothalamus) III. Hepatic (volume sensor, Na sensor)
Vascular Low-Pressure Volume Sensors • located within the walls of the cardiac atria, right ventricle, and large pulmonary vessels, and they respond to distention of these structures • The activity of these sensors modulates both sympathetic nerve outflow and ADH secretion. • The myocytes of the atria synthesize ,atrial natriuretic peptide (ANP) and BNP
Signals Involved in Control of Renal NaCl and Water Excretion Renal Sympathetic Nerves (↑ Activity: ↓ NaCl Excretion) • ↓ GFR • ↑ Renin secretion • ↑ Na+ reabsorption along the nephron Renin-Angiotensin-Aldosterone (↑ Secretion: ↓ NaCl Excretion) • ↑ Angiotensin II stimulates reabsorption of Na+ along the nephron • ↑ Aldosterone stimulates Na+ reabsorption in the thick ascending limb of Henle's loop, distal tubule, and collecting duct • ↑ Angiotensin II stimulates secretion of ADH
Natriuretic Peptides: ANP, BNP, and Urodilatin(↑ Secretion: ↑ NaCl Excretion) • ↑ GFR • ↓ Renin secretion • ↓ Aldosterone secretion (indirect via ↓ in angiotensin II and direct on the adrenal gland) • ↓ NaCl and water reabsorption by the collecting duct • ↓ ADH secretion and inhibition of ADH action on the distal tubule and collecting duct ADH (↑ Secretion: ↓ H2O Excretion) ↑ H2O reabsorption by the distal tubule and collecting duct
Chloride • Cl moves relatively easily between the extracellular and intracellular compartments because most plasma membranes contain many Cl leakage channels and antiporters
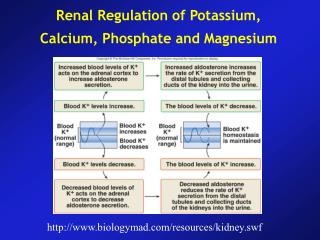
Potassium • Potassium ions are the most abundant cations in intracellular fluid (140 mEq/liter). • The normal blood plasma K+ concentration is 3. 5–5.0 mEq/liter and is controlled mainly by aldosterone. • K+ plays a key role in establishing the resting membrane potential and in the repolarization phase of action potentials in neurons and muscle fibers
K+ Functions Regulation of cell volume, regulation of intracellular pH, synthesis of DNA and protein, growth, enzyme function, resting membrane potential, cardiac and neuromuscular activity.
Extracellular Potassium Concentration and Cell Membrane Potential • Membrane potential ln[K]o [K]i +30 0 Depolarization - 30 Hyperpolarization mV - 60 Threshold Resting - 90 - 120 Normal Hypokalemia Hyperkalemia Hypokalemia hyperpolarizes excitable tissues Hyperkalemia depolarizes excitable tissues
ALKALEMIA H+ H+ H+ H+ K+ K+ K+ K+ ACID-BASE imbalance ACIDEMIA
[K+] Pancreas Insulin Liver [K+] K+ Muscle Potassium Homeostasis: Insulin • Insulin stimulates the cellular uptake of potassium via an increase in Na+,K+-ATPase activity
REGULATION OF K+ SECRETION BY THE DISTAL TUBULE AND COLLECTING DUCT
Hyperkalemiastimulates Na+,K+-ATPase and thereby increases K+ uptake across the basolateral membrane. This uptake raises intracellular [K+] and increases the electrochemical driving force for exit of K+ across the apical membrane. • Second, hyperkalemia also increases the permeability of the apical membrane to K+. • Third, hyperkalemia stimulates secretion of aldosterone by the adrenal cortex • Fourth, hyperkalemia also increases the flow rate of tubular fluid,
(-) 3 Na+ Na+ 2 K+ ENaC MR K+ ROMK Aldo Aldo Principal Cell Aldosterone Effects on the Principal Cell Regulation of K+ secretion by principal cells in the collecting duct is the primary basis for K+ homeostasis • Na+ reabsorption via Na+ channels (ENaC) results in a lumen-negativetranscellular potential difference • Lumen-negative potential difference favors K+ secretion via K+ channels (ROMK) Aldosterone • Aldosterone stimulates K+ secretion by principal cells in the collecting duct • Aldosterone binds to an intracellularreceptor, which when activated functions as a transcriptional regulator synthesis of aldosterone-induced proteins
2 K + ENaC Channel 3 Na + Na + Tubule Lumen K + Principal Cell ROMK Channel Apical Basolateral Distal Renal K+ Secretion:The Principal Cell in the Collecting Duct Major determinants of K+ secretion in the collecting duct • These K+ and Na+ transport processes are stimulated by aldosterone
Apical Basolateral 3 Na + ~ H + ~ 2 K + K + K + HCO - 3 H + ~ Cl - Intercalated Cell Cl - Distal Renal K+ Reabsorption:The Intercalated Cell in the Collecting Duct Potassium reabsorption by the intercalated cell is an active process which is mediated by the apical membrane H+,K+-ATPase
Distal Tubular Flow Rate Effects Potassium Secretion • increased tubular flow rate, • the secreted potassium is continuously flushed down the tubule, • so that the rise in tubular potassium concentration becomes minimized. • Therefore, net potassium secretion is stimu-lated by increased tubular flow rate
Acidosis • Acute acidosis leads to decreased potassium excretion whereas chronic acidosis leads to a loss of potassium
Calcium • The normal concentration of free or unattached Ca 2+ in blood plasma is 4.5–5.5 mEq/liter. About the same amount of Ca is attached to various plasma proteins. • Besides contributing to the hardness of bones and teeth, Ca2+plays important roles in blood clotting, neurotransmitter release, maintenance of muscle tone, and excitability of nervous and muscle tissue. • The most important regulator of Ca2+concentration in blood plasma is parathyroid hormone (PTH)
Parathyroid hormone (PTH) inhibits phosphate reabsorption in the proximal tubule by activating adenylate cyclase, generating cyclic AMP (cAMP), and inhibiting Na+-phosphate cotransport. • Thus, PTH increases urinary excretion of phosphate and lowers blood phosphate level. • Calcitriol promotes absorption of both phosphates and calcium from the gastrointestinal tract.
Magnesium • More than one half of the body’s magnesium is storedinthe bones. • Mg 2+is a cofactor for certain enzymes needed for the metabolism of carbohydrates and proteins and for the sodium–potassium pump. • Mg 2+is essential for normal neuromuscular activity, synaptic transmission, and myocardial functioning. • In addition, secretion of parathyroid hormone (PTH) depends on Mg2+
Regulation of magnesium excretion is achieved mainly by changing tubular reabsorption. • The proxi-mal tubule usually reabsorbs only about 25 per cent of the filtered magnesium. • The primary site of reabsorp-tion is the loop of Henle, where about 65 per cent of the filtered load of magnesium is reabsorbed
kidneys increase urinary excretion of Mg2in response to hyper-calcemia, hypermagnesemia, increases in extracellular fluid volume, decreases in parathyroid hormone, and acidosis. • The opposite conditions decrease renal excretion of Mg2