Download
1 / 27
270 likes | 437 Views
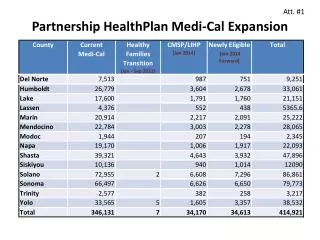
Partnership HealthPlan of California. Programs to Improve Care. Robert Moore, MD MPH Chief Medical Officer. Aligned Values. Quality Access Value Provider satisfaction Member satisfaction Serving the community. Improving Care. Quality Programs Care Coordination Programs.

E N D
Partnership HealthPlan of California Programs to Improve Care Robert Moore, MD MPH Chief Medical Officer
Aligned Values • Quality • Access • Value • Provider satisfaction • Member satisfaction • Serving the community
Improving Care • Quality Programs • Care Coordination Programs Partnership HealthPlan of California
Quality Programs • Quality Improvement Incentive Program (Pay for Performance) • Quality Assurance Programs • Peer Review • Data Analysis and Feedback • QI Projects • Convening of peer networks/collaborative learning efforts/educational events • Cultural and Linguistic Quality
Quality Improvement Incentive Program • Principles • Types • Categories • Funds: Compared to other plans. • Related to PPS • Related to PCMH Measures. • An Example
QIP Principles • Collaboration with Providers • Simplicity in the number of measures • Actionable • Feasible data collection • Sizeable Incentives • Comprehensive measurement set • Align measures that are meaningful • Pay for Exceptional Performance and Improvement • Stable measures • Distribute 100% of Fixed PMPM Funds
QIP types • Fixed Pool PMPM • Set amount of dollars • All dollars given out • One provider’s low performance means more money to higher performers • Unit of Service Measures • Payment for completion of Project • Payment for discrete actions
QIP Categories • Clinical Measures: 35% • Appropriate Use of Resources: 35% • Access: 20% • Patient Experience: 10%
Size of the QIP • Largest of any HealthPlan in California • 5 other County Organized Health Systems • 10 Local Initiatives • 5 Private HealthPlans
Alignment with PCMH • 51% of points of fixed pool PMPM are for measures that impact PCMH status • 8 out of 9 unit of service measures are related to PCHH
How is PPS affected? • How does Capitation affect PPS? • How does fee for service affect PPS? • How does Quality Improvement Incentive Program affect PPS? • How do risk pool payments affect PPS?
QIP example: Medium Sized FQHC: Visit Income • Health Center Budget: $500,000 per month ($6 million/yr) • “Unfavorable” Payer mix: 25% Partnership MediCal • About 4000 Capitated Patients: 70% Adults, 30% Children • Capitation Check: About $50,000 per month • Visits per month: • 1000 by Capitated Patients • 400 by “Special Members” (Non-capitated): Paying $30 per visit • PPS Rate: $150 per visit • Total Monthly Income from PPS Visits: $210,000 • Balance of PPS Rate Paid by State: • $210K-$50K-12K / 1400 Visits= $105 per visit
QIP example:Medium Sized FQHC: Other income • Not subject to PPS limit: • QIP: Fixed Pool: $4 PMPM allocated • 100% of points awarded • Average score of all providers 80% • Effective payout $4.80 PMPM • Equal to $230,400 per year, or $19,200 per month • Other QIP Income: • $66,000 per year or $5500 per month • Special Member Risk Pool: • $48,000 per year or $4000 per month
QIP ExampleMedium Sized FQHC: Grand total • Visit Income from Cap: $50,000 per month • Other Income from PHC: $28,700 per month • PPS wraparound from state: $160,000 per month • Total $238,700 per month • $170.50 per visit • 48% of budget
QIP ExampleMedium Sized Health Center • Investing QIP money: • Staff incentive or reward program • Hire chronic disease case managers • Women’s health • Diabetes • Allocate staff time to QIP activities: • In-reach • Organizing forms • Provider and Staff Education on Topics affecting QIP • Reviewing list of patients that went to Emergency Room each Day • Case managing patients in hospital/discharged from hospital • Data Analysis • QIP coordinating committee
Care Coordination Activities • Transportation Benefit • Growing Together Program (Perinatal) • Care Transitions • Case Management • Complex Case Management (telephonic) • Intensive Case Management (in-person) • Home Visiting Nurse Practitioner Program
Drivers of high hospital costs • Top 1-5% of patients by total cost drive most hospital costs • Inappropriate care in severely ill individuals • Excess specialty care • Patients with poorly controlled substance abuse, mental health problems with serious chronic medical illness • Major theme: need better care and more coordination
Severity-specific Care Coordination Clinician home visits, reliable on call Homebound, frail, labile health, very high costs 0.1% Frequent hospitalizations, medical and behavioral issues Intensive case management 3% Chronically Ill, 3 modifiable conditions Complex Case Management 7% Need specific, short-term support Case Management 20% Well, or stable chronic illness Primary Care 70%
Case I: 50 yo woman from Vallejo • Health Plan Contracted outside FNP agency • Home Visit Based • Home Bound patient
Barriers to Care Coordination for patients at home • Clinic culture that is provider-centric instead of patient centric • Unable to come up with system to pay for home care • Links with ER doctors and hospitalists
Case Study II: 40 yo woman with diabetes • Plan based telephonic case management • Nurse-navigator teams • Remote care, patient at home
Intensive Case Management – Evidence Base • Atul Gawande’s “Hot Spotters” article • Care Oregon’s case managers embedded in PCP office/clinic • Monarch Health: non-integrated “high-risk touch team” • HealthCare Partners: Embedded Complex Case Management • Wellpoint: pay for care plan submission
Intensive Case Management • Contracted Services Model: • $100,000 of funding to the health center/clinic which will hire, train and oversee case manager. • Embedded Case Manager Model: • Partnership HealthPlan Hires a Case manager who will be embedded in the health center/clinic • $5,000 of funding to health center/clinic to cover collateral expenses. • Integrated Care Team Case Management: • $100,000 of funding to support training many case managers, each based in a primary care team • All Models: • focusing on 50 high-cost and complex patients who are primary care patients at the health center/clinic
Intensive Case Management Principles • Funded through Payer, by savings • Reduce Readmissions and Inappropriate Admissions • Target highest cost patients • Work with PCP • In person case management • Accountability: Care Plan submission
Role of Integrators in triple aim • Micro integrator • Macro integrator
Questions? Partnership HealthPlan Leadership Team