Download
1 / 18
190 likes | 2.07k Views
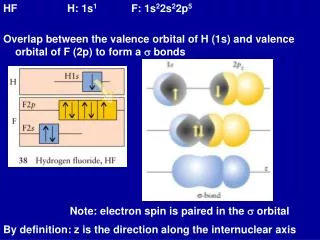
Orbital Pseudotumor: Idiopathic Orbital Inflammation. Shiva Kambhampati MS4,George Washington University School of Medicine/ University of North Carolina at Chapel Hill . Outline. What is Orbital Pseudotumor? Differential Diagnosis Case Presentation Radiological Findings and Analysis

E N D
Orbital Pseudotumor:Idiopathic Orbital Inflammation Shiva Kambhampati MS4,George Washington University School of Medicine/ University of North Carolina at Chapel Hill
Outline • What is Orbital Pseudotumor? • Differential Diagnosis • Case Presentation • Radiological Findings and Analysis • Orbital Pseudotumor Subtypes • Treatment • Conclusions
What is Orbital Pseudotumor? • First described in the 1900s • AKA “Idiopathic Orbital Inflammation”, or “nonspecific Orbital Inflammatory Disease” • Nonmalignant space occupying lesion involves orbital tissue and simulates a neoplasm • Diagnosis of exclusion, based on patient history, clinical picture, response to steroids, and occasionally by biopsy • Etiology unknown • 3rd most common cause of orbital inflammation
Differential Diagnosis of Orbital Inflammation • Inflammatory • Thyroid Opthalmopathy • Sarcoidosis • Wegener’s • Orbital Cellulitis • Abscess • Vasculitis • Neoplastic • Lymphoma • Metastases
Clinical Presentation • Typically acute – but can be insidious • Painful • Usually unilateral • No real pattern of muscle involvement • Ocular findings include: • Diplopia • Decreased Visual Acuity • Proptosis • Edema • Absent systemic symptoms
Imaging Findings of Orbital Pseudotumor • Imaging findings are characterized by inflammatory changes in orbital structures such as globe, lacrimal glands, extraocular muscles, orbital fat, and the optic nerve. • MR findings: • Isointense on T1 • Hypointense compared to normal muscle on T2 • Enhancement on post-contrast T1 images
Case Presentation • 62 y-o male dull ache in left eye and limited EOM • PMH: uveitis • Other Classical Clinical Presentations include: • Eye pain • Edema • Proptosis • Motility Restriction • Ophthalmoplegia • Lid Erythema
Case: Axial T1 Pre-Contrast Axial T1 image shows isointense infiltrative process in left eye involving the retro-ocular fat and external rectus muscle.
Case: Axial T2 Axial T2 image shows the process to be mostly hypointense. Note proptosis.
Case: Axial T1 Post-Contrast Post contrast T1 image shows the process to enhance and extend to ipsilateral cavernous sinus and along dura of left middle cranial fossa.
Orbital Pseudotumor Forms • Dacryoadenitis • Myositis • Sclerosis • Optic Nerve involvement • Tolosa-Hunt Syndrome • Intracranial extension
Differential Diagnosis of Orbital Inflammation • Inflammatory • Thyroid Opthalmopathy • Sarcoidosis • Wegener’s • Orbital Cellulitis • Abscess • Vasculitis • Neoplastic • Lymphoma • Metastases
Histology of Idiopathic Orbital Inflammation • Fibrous connective tissue and scant perivascular patchy polyclonal lymphocytic infiltrates
Treatment • Systemic Corticosteroids • Usually rapid clinical response and resolution of pain • Radiotherapy • 2nd line therapy • Adjuvant treatment when incomplete response • 1st line therapy if steroids contraindicated • Immunomodulators/Immunosuppresants
Conclusions • Fairly common cause of orbital inflammation (3rd) • Diagnosis of Exclusion, other causes must be ruled out • Occasionally diagnosis by biopsy is performed • Systemic Corticosteroids is primary treatment • Rapid response to steroid treatment supports diagnosis of Orbital Pseudotumor • MRI better imaging modality for characterizing intracranial extension • Orbital Pseudotumor is not a lymphoid tumor
Etiology • Etiology of Idiopathic Orbital Pseudotumor is unknown, but there are some theories in the literature • Originally it was thought to be infectious in origin, with historical reports occurring after viral illnesses. • Autoimmune pathogenesis was theorized because of a strong association with and rheumatologic diseases. • Reports of circulating antibodies against extraocular muscle proteins • IgG4 Related Systemic Disease • Theory that links different inflammatory disorders that were previously thought to be unrelated
IgG4 Related Systemic Disease (IgG4-RSD) • Systemic disease that is characterized by extensive IgG4-positive plasma cells and T-lymphocyte infiltration of various organs • Pancreatitis, sclerosing cholangitis, cholecystitis, sialadenitis, retroperitoneal fibrosis, tubulointerstitial nephritis, interstitial pneumonia, prostatitis, inflammatory pseudotumor and lymphadenopathy, are all thought to be IgG4-related • The prototype is IgG4-related sclerosing pancreatitis (also known as autoimmune pancreatitis) • Disease usually responds well to steroid therapy
References • Yuen SJ, Rubin PA. Idiopathic orbital inflammation: distribution, clinical features, and treatment outcome. Arch Ophthalmol 2003;121:491-9. • Lee et al. MR Imaging of Orbital Inflammatory Pseudotumors with Extraorbital Extension. Korean J Radiol. 2005 Apr-Jun; 6(2): 82–88. • Bencherif B, Zouaoui A, Chedid G, Kujas M, Van Effenterre R, Marsault C. Intracranial extension of an idiopathic orbital inflammatory pseudotumor. AJNR Am J Neuroradiol. 1993;14:181–184.[PubMed] • Weber AL, Romo LV, Sabates NR. Pseudotumor of the orbit. Clinical, pathologic, and radiologic evaluation. RadiolClin North Am. 1999;37:151–168. [PubMed] • Maksimovic O, Bethge WA, Pintoffl JP et-al. Marginal zone B-cell non-Hodgkin's lymphoma of mucosa-associated lymphoid tissue type: imaging findings. AJR Am J Roentgenol. 2008;191 (3): 921-30. doi:10.2214/AJR.07.2629 • Cheuk W. IgG4-related sclerosing disease: a critical appraisal of an evolving clinicopathologic entity. Advances in Anatomic Pathology. 2010 Sep;17(5):303-32.