Download

1 / 28
280 likes | 1.1k Views
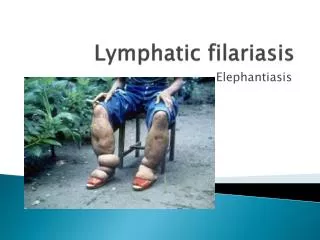
Epidemiology and Clinical Manifestations of Lymphatic Filariasis. Dr. Dilip Kumar Das Associate Professor, Community Medicine R. G. Kar Medical College, Kolkata, West Bengal. What is Lymphatic Filariasis?.

E N D
Epidemiology and Clinical Manifestations of Lymphatic Filariasis Dr. Dilip Kumar Das Associate Professor, Community Medicine R. G. Kar Medical College, Kolkata, West Bengal
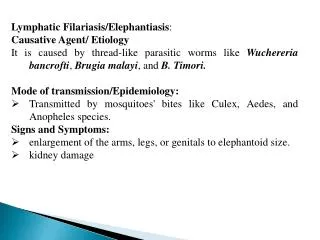
What is Lymphatic Filariasis? • Lymphatic filariasis is a disfiguring, disabling communicable human disease caused by the thread like nematode parasitic filarial worms. • A leading cause of permanent and long-term disability in the world • A cause of major social and economic burden
Globally……… • Affects 83 countries in the world • About 1.2 billion people at risk of infection • 120 million people have some form of the disease • 40 million are incapacitated/disfigured • SEAR: 60 million infected, 31 million have clinical manifestations • More than one third of the infected people in India
Filarial Endemicity in India Endemic districts with MF rate 1% and above Low endemic districts with MF rate below 1% Districtsunder survey Non-endemic districts
In India……. • 250 districts in 20 states/UTs are endemic • 600 million people are at risk of infection • 6 million attacks of acute filarial disease per year • 20 million one or more chronic filarial lesions • Highly endemic states: Uttar Pradesh, Bihar, Jharkhand, Andhra Pradesh, Orissa, Tamilnadu, Kerala, Gujarat.
Basic Epidemiology of LF Agent : • Filarial parasite: Nematode • 3 of 8 species cause Lymphatic Filariasis • Wuchereriabancrofti, Brugiamalayi, Brugiatimori • In India: W. bancrofti (99.4%) and B. malayi (0.6%) cause LF • Develops in two hosts: Man – Primary (definitive) host Mosquito – Secondary (intermediate) host Periodicity Nocturnally Periodic Diurnally Sub-periodic
Basic Epidemiology of LF… Host : - Man is the natural host. - All ages are susceptible to infection. - Adults are more frequently and more heavily infected than children - Mf rate is higher in men - Filaria disease appears in a small percentage of infected individuals. - Urbanization, industrialization, migration of people and specific habits are some of the social factors associated with filariasis.
Basic Epidemiology of LF… Vectors : • BancroftianFilariasis (nocturnally periodic): Culexquinquefasciatus. • Brugian (Malayan) Filariasis: Mansonoidesannulifera, M. uniformis, M. indiana. • BancroftianFilariasis (Diurnally sub-periodic): Ochlarotatus (Finlaya) niveus group • C. quinquefasciatus generally breed in dirty and polluted water (stagnant drains, cesspools, septic tanks, burrow pits etc). Mansonoides breed in water bodies containing certain aquatic plants • C. quinquefasciatus is highly anthrophilic, an indoor rester (endophilic) and bites at midnight.
Basic Epidemiology of LF… Environment: • Prevalent both in urban and rural areas • Climate influences the breeding and longevity of vector mosquitoes and also determines the development of parasite in the vector • Bad drainage, inadequate sewage disposal, lack of town planning increase vector breeding
Incubation Period • Extrinsic incubation period: Time interval for microfilariae to develop inside the mosquito to 3rd stage infective larvae. (10 – 14 days) • Pre-patent period: Time interval between introduction of infective larvae and the first appearance of detectable Mf in the peripheral blood. (12 –18 months) • Clinical incubation period: Time interval from invasion of infective larvae to the development of clinical manifestations. (8 – 16 months)
Clinical Manifestations • Lymphatic Filariasis • Stage of invasion • Asymptomatic/carrier stage • Stage of acute manifestations • Stage of chronic manifestations • Ocult Filariasis
Clinical features • Recurrent attacks • Filarial fever • Lymphangitis • Lymphadenitis • Epididymo-orchitis in males • Mastitis in females • Lymphoedema • Elephantiasis • Hydrocele • Chyluria
Entry lesions common in Lymphoedema InjuryCandidiasis PyodermaParonychia Fissure foot Eczema Insect bites
LF is a social evil… Disfigurement of limbs and genitalia leads to • Stigma • Anxiety • Ostracization • Psychological trauma • Sexual dysfunction The disease impedes • Mobility • Travel • Educational opportunities • Employment opportunities • Marriage prospects
Global economic loss at US $ 2 billion per annum India loses 1.2 billion man days annually Estimated economic loss in India alone is US $ 850 million per year The economic loss is equivalent to 0.05% of GNP A major cause of poverty in the regions LF drains the economy…
How can LF be diagnosed? • Clinical examination for filarial symptoms • Detection of microfilariae in mf carriers - Thick blood film (20 c.mm) microscopy at night (8-30 PM – 12 AM) - MFC method - DEC provocation test • Antigen detection Immunochromatographic test (ICT): Field friendly, sensitive and specific, easy to perform and can be done at any time during the day or night • DNA based molecular techniques
Filaria Survey Prevalence of Filariasis can be estimated by • Clinical Survey • Parasitological Survey • Entomological Survey
Parasitological indices • Microfilaria rate: No of slides +ve for mf Total number of slides examined • Average mf density Total number of mf among +ve blood smears Number of +ve blood smears • Disease rate No of persons +ve for disease Total number of persons examined x 100 x 100
Entomological indices • 10 man hour density No of male & female Cx. Quinquefasciatus collected Time (in hours) spent on mosquito collection • Vector infection rate - Percentage of female vector mosquitoes +ve for L-1/L-2/ L-3 stage larvae • Vector infectivity rate - Percentage of female vector mosquitoes +ve for infective larvae (L-3 stage) • Average number of infective larvae per infective mosquito x 10