Download
1 / 71
710 likes | 833 Views
Screening and Assessment: Lessons from RWJF’ s Reclaiming Futures Projects. Michael Dennis, Ph.D. Chestnut Health Systems, Bloomington, IL

E N D
Screening and Assessment: Lessons from RWJF’ s Reclaiming Futures Projects Michael Dennis, Ph.D. Chestnut Health Systems, Bloomington, IL On line webinar Presentation for Reclaiming Futures, March 28, 2009. This presentation was supported by a Grant from the Robert Woods Johnson Foundation (RWJF) and reports on treatment & research funded by them as well as Center for Substance Abuse Treatment (CSAT), Substance Abuse and Mental Health Services Administration (SAMHSA) under contracts 270-2003-00006 and 270-07-0191, as well as several individual CSAT, NIAAA, NIDA and private foundation grants. The opinions are those of the author and do not reflect official positions of the consortium or government. Available on line at www.chestnut.org/LI/Posters or by contacting Michael Dennis, Chestnut Health Systems, 448 Wylie Drive, Normal, IL 61761, phone 309-451-7801, fax 309-451-7765, e-Mail: mdennis@Chestnut.Org Questions about the GAIN can also be sent to gaininfo@chestnut.org
Goals of this Presentation are to • Summarize the physical and chronic nature of substance use disorders, why the justice system cares and why adolescence is just a critical time period • Describe the need for standardizing how we identify juveniles with behavioral health issues • Explaining how to decide what is needed on the continuum of screening to assessment • Illustrate how the differences in what this looks like in terms what you receive at client and program level using data from 5 of the original Reclaiming Futures Sites • Discuss implications for program planing and policy
Short Term Impact of Substance Use on the Brain (PET Scan Minutes After Using Cocaine) Rapid rise in brain activity after taking cocaine Actually ends up lower than they started Photo courtesy of Nora Volkow, Ph.D. Mapping cocaine binding sites in human and baboon brain in vivo. Fowler JS, Volkow ND, Wolf AP, Dewey SL, Schlyer DJ, Macgregor RIR, Hitzemann R, Logan J, Bendreim B, Gatley ST. et al. Synapse 1989;4(4):371-377.
Recovery from cumulative use takes more time (PET Scan Activity Days After Using Cocaine) With repeated use, there is a cumulative effect of reduced brain activity which requires increasingly more stimulation (i.e., tolerance) Normal Cocaine Abuser (10 days) Even after 100 days of abstinence activity is still low Cocaine Abuser (100 days) Photo courtesy of Nora Volkow, Ph.D. Volkow ND, Hitzemann R, Wang C-I, Fowler IS, Wolf AP, Dewey SL. Long-term frontal brain metabolic changes in cocaine abusers. Synapse 11:184-190, 1992; Volkow ND, Fowler JS, Wang G-J, Hitzemann R, Logan J, Schlyer D, Dewey 5, Wolf AP. Decreased dopamine D2 receptor availability is associated with reduced frontal metabolism in cocaine abusers. Synapse 14:169-177, 1993.
The effects on the brain can be long lasting(Serotonin Present in Cerebral Cortex Neurons ) Still not back to normal after 7 years Reduced in response to excessive use Image courtesy of Dr. GA Ricaurte, Johns Hopkins University School of Medicine
The Costs of Substance Use • Drug use costs the U.S. over $181 billion a year, primarily due to productivity loss, and health care and crime costs (Harwood, 2000) • Abuse of alcohol, tobacco, and other drugs, kills more Americans than any other class of health behavior (Mokdad et al 2004) • Of the 20,196 deaths from overdose in 2004, 358 (2%) were from alcohol and 19,838 (98%) were from other drugs, with 9798 (49%) from opioids. (MMWR, 2007) • Of the 23.2 million people (9.5% of the U.S. population) who had substance disorders in 2005, only 2.2 million (0.9%) received any treatment (OAS, 2006)
Overlap with Crime and Civil Issues • Committing property crime, drug related crimes, gang related crimes, prostitution, and gambling to trade or get the money for alcohol or other drugs • Committing more impulsive and/or violent acts while under the influence of alcohol and other drugs • Crime levels peak between ages of 15-20 (periods or increased stimulation and low impulse control in the brain) • Adolescent crime is still the main predictor of adult crime • Parent substance use is intertwined with child maltreatment and neglect – which in turn is associated with more use, mental health problems and perpetration of violence on others
Potential Cost Savings of Expanding Diversion to Treatment Programs in Justice Settings • Currently treating about 55,000 people in these diversion programs and drug courts at a cost of $515 million with an average return on investment (ROI) of $2.14 per dollar • The ROI is higher (2.71) for those with more crime • It is estimated that there are at least twice as many people in need of drug court as getting it • Investing the $1 billion to treat them would likely produce a ROI of $2.17 billion to society Source: Bhati et al (2008) To Treat or Not To Treat: Evidence on the Prospects of Expanding Treatment to Drug-Involved Offenders. Washington, DC: Urban Institute.
Adolescent Onset Remission Severity of Past Year Substance Use/Disorders by age NSDUH Age Groups Increasing rate of non-users 100 Severity Category 90 No Alcohol or Drug Use 80 70 Light Alcohol Use Only 60 Any Infrequent Drug Use 50 40 Regular AOD Use 30 Abuse 20 10 Dependence 0 (2002 U.S. Household Population age 12+= 235,143,246) 65+ 12-13 14-15 16-17 18-20 21-29 30-34 35-49 50-64 Source: 2002 NSDUH; Dennis & Scott 2007
Severity is related to other violence/crime problems Crime & Violence by Substance Severity Age 12-17 Source: NSDUH 2006
Family, Vocational & MH by Substance Severity Age 12-17 As well as other School and Mental Health Problems Source: NSDUH 2006
Main reasons for using are to get pleasure or dull pain pain Adolescent Brain Development Occurs from the Inside to Out and from Back to Front Photo courtesy of the NIDA Web site. From A Slide Teaching Packet: The Brain and the Actions of Cocaine, Opiates, and Marijuana.t
Substance Use Careers Last for Decades 1.0 Median of 27 years from first use to 1+ years abstinence .9 Cumulative Survival .8 .7 Years from first use to 1+ years abstinence .6 .5 .4 .3 .2 .1 0.0 0 5 10 15 20 25 30 Source: Dennis et al., 2005
Substance Use Careers are Longer the Younger the Age of First Use Age of 1st Use Groups 1.0 .9 .8 Cumulative Survival .7 Years from first use to 1+ years abstinence .6 .5 under 15* .4 15-20* .3 .2 21+ .1 0.0 * p<.05 (different from 21+) 0 5 10 15 20 25 30 Source: Dennis et al., 2005
Substance Use Careers are Shorter the Sooner People Get to Treatment Year to 1st Tx Groups 1.0 .9 .8 Cumulative Survival .7 Years from first use to 1+ years abstinence 20+ .6 .5 .4 Reducing the years of use and its associated problems by over a decade .3 10-19* .2 .1 0.0 0-9* * p<.05 (different from 20+) 0 5 10 15 20 25 30 Source: Dennis et al., 2005
Treatment Careers Last for Years Median of 3 to 4 episodes of treatment over 9 years 1.0 .9 Cumulative Survival .8 Over 2/3rds eventually get better (which is better than most major DSM disorders) .7 Years from first Tx to 1+ years abstinence .6 .5 .4 .3 .2 .1 0.0 0 5 10 15 20 25 Source: Dennis et al., 2005
Several Recent Reviews and over 22 Experiments and Quasi-Experiments Have Demonstrated That A growing range of drug treatment courts are being found effective and cost effective More assertive continuing care can increase adherence with continuing care expectations Recovery management checkups can identify people who have relapsed and get them back to treatment faster That doing each improves short and long term outcomes That the rate of improve effects went up as interventions when from less than 3 months (38%) to 3 to 12 months (44%) to more than 12 months (100%) Source: Bhati et al 2008; Dennis et al 2003, 2007, Godley et al 2002, 2007; Marlowe, 2008; McKay, in press; Scott et al 2005, in press
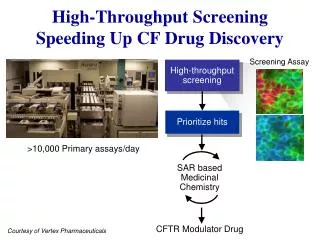
The Movement to Increase Screening • Screening, Brief Intervention and Referral to Treatment (SBIRT) has been shown to be effective in identifying people not currently in treatment, initiating treatment/change and improving outcomes (see http://sbirt.samhsa.gov/ ) • The US Preventive Services Task Force (USPSTF, 2004; 2007), National Quality Forum (NQF, 2007), and Healthy People 2010 have each recommended regular screening, brief intervention, and referral to treatment (SBIRT) for tobacco and alcohol abuse in general medical settings for everyone • The latter two also recommend SBIRT for drug use in high risk populations (e.g., adolescents, pregnant and post partum women, people with HIV, and people with co-occurring psychiatric conditions) • RWJF, OJJDP, CSAT and NIDA are each funding several projects to develop and evaluate models for doing this
Places vary in the rate of problems (Past Year Substance Abuse or Dependence) There is even variation within DC (an area less than 10 square miles) and of course within individuals Source: OAS, 2006
Crime/ Violence predicted recidivism Substance Problem Severity predicted recidivism Knowing both was the best predictor Crime/Violence and Substance Problems Interact to Predict Any Recidivism 12 month recidivism 100% 80% 60% 40% 20% Crime and Violence Scale Substance Problem Scale 0% High High Mod. Mod. Low Low Source: CYT & ATM Data
100% 80% Crime/ Violence predicted violent recidivism 60% 40% 20% 0% Knowing both was the best predictor Crime/Violence and Substance Problems Interact Differently to Predict Recidivism to Violent Crime 12 month recidivism To violent crime or arrest Crime and Violence Scale Substance Problem Scale High High Mod. Mod. (Intake) Substance Problem Severity did not predict violent recidivism Low Low Source: CYT & ATM Data
Mental Health Comorbidity Among Girls in Detention Multiple Problems are the norm Source: Teplin, LA, Abram, KM, McCelland, GM, Mericle, AA, Dulcan, MK, and Washburn, JJ (2006) Psychiatric Disorders of Youth in Detention. Washington, DC: OJJDP. Retrieved from http://www.ncjrs.gov/pdffiles1/ojjdp/210331.pdf
Mental Health Comorbidity Among Boys in Detention While there are gender differences, the differences are often degrees of variation Source: Teplin, LA, Abram, KM, McCelland, GM, Mericle, AA, Dulcan, MK, and Washburn, JJ (2006) Psychiatric Disorders of Youth in Detention. Washington, DC: OJJDP. Retrieved from http://www.ncjrs.gov/pdffiles1/ojjdp/210331.pdf
Number of Major Clinical Problems by System of Care * (Alcohol, cannabis, or other drug disorder, depression, anxiety, trauma, suicide, ADHD, CD, victimization, violence/ illegal activity) Source: Dennis et al in 2008; CSAT 2007 AT Outcome Data Set (n=12,824)
Number of Problems is Related to Level of Care Clients entering Short Term Residential (usually dual diagnosis) have 5.5 times higher odds of having 5+ major problems* * (Alcohol, cannabis, or other drug disorder, depression, anxiety, trauma, suicide, ADHD, CD, victimization, violence/ illegal activity) Source: Dennis et al 2009; CSAT 2007 Adolescent Treatment Outcome Data Set (n=12,824)
No. of Prob. is related to the Severity of Victimization Those with high lifetime levels of victimization have 13 times higher odds of having 5+ major problems* Severity of Victimization * (Alcohol, cannabis, or other drug disorder, depression, anxiety, trauma, suicide, ADHD, CD, victimization, violence/ illegal activity) Source: Dennis et al 2009; CSAT 2007 Adolescent Treatment Outcome Data Set (n=12,824)
Continuum of Measurement (Common Measures) More Extensive / Longer/ Expensive Screener Quick Comprehensive Special • Screening to Identify Who Needs to be “Assessed” (5-10 min) • Focus on brevity, simplicity for administration & scoring • Needs to be adequate for triage and referral • GAIN Short Screener for SUD, MH & Crime • ASSIST, AUDIT, CAGE, CRAFT, DAST, MAST for SUD • SCL, HSCL, BSI, CANS for Mental Health • LSI, MAYSI, YLS for Crime • Quick Assessment for Targeted Referral (20-30 min) • Assessment of who needs a feedback, brief intervention or referral for more specialized assessment or treatment • Needs to be adequate for brief intervention • GAIN Quick • ADI, ASI, SASSI, T-ASI, MINI • Comprehensive Biopsychosocial (1-2 hours) • Used to identify common problems and how they are interrelated • Needs to be adequate for diagnosis, treatment planning and placement of common problems • GAIN Initial (Clinical Core and Full) • CASI, A-CASI • Specialized Assessment • Additional assessment by a specialist (e.g., psychiatrist, MD, nurse, spec ed) may be needed to rule out a diagnosis or develop a treatment plan or individual education plan • CIDI, DISC, KSADS, PDI, SCAN
Key Work Force / System Issues to Consider When Selecting Assessment • High turnover workforce with variable educationbackground related to diagnosis, placement and treatment planning. • Heterogeneous needs and severitycharacterized by multiple problems, chronic relapse, and multiple episodes of care • Lack of access to or use of data at the program levelto guide immediate clinical decisions, billing and program planning • Missing or misrepresented datathat needs to be minimized and incorporated into interpretations
Global Appraisal of Individual Needs (GAIN) Logic Model as an Example Issue Instrument Feature Protocol Feature Outcome • Standardized approach to asking questions across domains • Questions spelled out and simple question format • Lay wording mapped onto expert standards for given area • Built in transition statements, prompts, and checks for inconsistent and missing information. • Responses to frequently asked questions • Multiple training resources • Formal training and certification protocols on administration, clinical interpretation, data management, project coordination, local, regional, and national “trainers” • Above focuses on consistency across populations, level of care, staff and time • On-going quality assurance and data monitoring for the reoccurrence or problems at the staff (site or item) level • Availability of technical assistance High Turnover Workforce with Variable Education Improved Reliability and Efficiency • Multiple domains • Focus on most common problems • Participant self description of characteristics, problems, needs, personal strengths and resources • Behavior recency, breadth, frequency • Utilization lifetime, recency and frequency • Dimensional measures • Interpretative cut points • Items and cut points mapped onto DSM for diagnosis, ASAM for placement, and to multiple standards and evidence- based practices for treatment planning • Computer generated scoring and reports • Treatment planning recommendations and links to evidence-based practice • Basic and advanced clinical interpretation training and certification Comprehensive Assessment Heterogeneous Needs and Severity
Global Appraisal of Individual Needs (GAIN) Logic Model as an Example Issue Instrument Feature Protocol Feature Outcome • Data immediately available to support clinical decision making for a case • Data can be transferred to other clinical information system to support billing, progress reports, treatment planning and on-going monitoring • Data can be exported and cleaned to support further analyses • Data can be pooled with other sites to facilitate comparison and evaluation • PC and (soon) web based software applications and support • Formal training and certification on using data at the individual level and data management at the program level • Data routine pooled to support comparisons across programs and secondary analysis • Over two dozen scientists working with data to link to evidence-based practice Lack of Access to or use of Data at the Program Level Improved Program Planning and Outcomes • Assurances, time anchoring, definitions, transition, and question order to reduce confusion and increase valid responses • Cognitive impairment check • Validity checks on missing, bad, inconsistency and unlikely responses • Validity checks for atypical and overly random symptom presentations • Validity ratings by staff • Training on optimizing clinical rapport • Training on time anchoring • Training answering questions, resolving vague or inconsistent responses, following assessment protocol and accurate documentation. • Utilization and documentation of other sources of information • Post hoc checks for on-going site, staff or item problems Missing or Misrepresented Data Improved Validity
Questions So Far? For the rest of the session we will focus on doing two things simultaneously • Demonstrating the difference in the depth and and breadth of information you get with different levels of assessment • Doing this by using findings from the first cohort of RWJF Reclaiming Future sites to also review what they learned
GAIN Clinical Collaborators Adolescent and Adult Treatment Program New Hampshire Washington Vermont North Maine Montana Dakota Minnesota Oregon Massachusetts South Wisconsin Idaho Dakota New York Michigan Wyoming Rhode Island Pennsylvania Iowa Connecticut Nebraska Ohio Nevada New Jersey Illinois Indiana Utah W. Virginia Delaware Colorado California Kansas Virginia Missouri Kentucky Maryland North Carolina Tennessee District Of Columbia Oklahoma New Mexico Arkansas Arizona South Carolina Number of GAIN Sites Mississippi Georgia 0 Alabama 1 to 10 Texas 11 to 25 Louisiana 26 to 130 Alaska GAIN State System Florida GAIN-SS State or County System Hawaii Virgin Islands Puerto Rico 10/08
Across measures, the GAIN has a Common Factor Structure of Psychopathology Source: Dennis, Chan, and Funk (2006)
GAIN-Short Screener (GSS): Overview • Administration Time: A 3- to 5-minute screener • Purpose: Used in general populations to • identify or rule-out clients who will be identified as having any behavioral health disorders on the 60-120 min versions of the GAIN • triage area of problem • serve as a simple measure of change • Easy for administration and interpretation by staff with minimal training or direct supervision • Mode: Designed for self- or staff-administration, with paper and pen, computer, or on the web • Translations: English, with translations with us into Spanish and by collaborators into several languages including French, Hmong, Japanese, Mandarin, Pilipino, Portuguese, and Vietnamese so far
GAIN-Short Screener (GSS): Overview (continued) • Scales: Four screeners for Internalizing Disorders, Externalizing Disorders, Substance Disorders, Crime/Violence, and a Total • Response Set: Recency of 20 problems rated past month (3), 2-12 months ago (2), more than a year ago (1), never (0) • Interpretation: Combined by cumulative time period as: • Past month count (3s) to measure of change • Past year count (2s or 3s) to predict diagnosis • Lifetime count (1s, 2s or 3s) as a measure of peak severity • Can be classified within time period low (0), moderate (1-2) or high (3) • Can also be used to classify remission as • Early (lifetime but not past month) • Sustained (lifetime but not past year) • Reports: Narrative, tabular, and graphical reports built into web based GAIN ABS and/or ASP application for local hosting
Internalizing Disorder Screening (IDScr) Externalizing Disorder Screening (EDScr)
Substance Disorder Screening (SDScr) Crime/violenceDisorder Screening (CVScr)
GAIN Short Screener Profile of 2 Recl. Futures Sites(Range based on 0/1-2/3+ Symptoms) Source: Reclaiming Futures Portland, OR and Santa Cruz, CA sites (n=192)
GAIN Short Screener Number of Problems Mod/Hi 93% endorsed one or more problems (40% 4 or more) Source: Reclaiming Futures Portland, OR and Santa Cruz, CA sites (n=192)
GAIN SS Psychometric Properties Low Mod. High 100% Prevalence (% 1+ disorder) 90% Sensitivity (% w disorder above) 80% Specificity (% w/o disorder below) 70% (n=6194 adolescents) 60% Using a lower cut point increases prevalence and specificity, but decreases sensitivity 50% 40% At 3 or more symptoms we get 99% prevalence, 91% sensitivity, & 89% specificity 30% 20% 10% 0% 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 Total Disorder Screener (TDScr) Total score has alpha of .85 and is correlated .94 with full GAIN version Source: Dennis et al 2006
GSS Performance by Subscale and Disorders Prevalence Sensitivity Specificity Screener/Disorder 1+ 3+ 1+ 3+ 1+ 3+ Low (0), Moderate (1-2), and High (3+) cut points can be used to identify the need for specific types of interventions Internal Disorder Screener (0-5) Any Internal Disorder 81% 99% 94% 55% 71% 99% Major Depression 56% 87% 98% 72% 54% 94% Generalized Anxiety 32% 56% 100% 83% 44% 83% Suicide Ideation 24% 43% 100% 84% 41% 79% Mod/High Traumatic Stress 60% 82% 94% 60% 55% 90% External Disorder Screener (0-5) Any External Disorder 88% 97% 98% 67% 75% 96% AD, HD or Both 65% 82% 99% 78% 51% 85% Conduct Disorder 78% 91% 98% 70% 62% 90% Substance Use Disorder Screener (0-5) Moderate can be targeted where resources allow or where a more assertive approach is desired Any Substance Disorder 96% 100% 96% 68% 73% 100% Dependence 65% 87% 100% 91% 30% 82% Abuse 30% 13% 89% 25% 14% 28% Crime Violence Screener (0-5) Any Crime/Violence 88% 99% 94% 49% 76% 99% High Physical Conflict 31% 46% 100% 70% 38% 77% Mod/High General Crime 85% 100% 94% 51% 71% 100% Total Disorder Screener (0-5) Mod/Hi can be used to evaluate program delivery/referral Any Disorder 97% 99% 99% 91% 47% 89% Any Internal Disorder 58% 63% 100% 98% 8% 28% Any External Disorder 68% 75% 100% 99% 10% 37% Any Substance Disorder 89% 92% 99% 92% 20% 51% Any Crime/Violence 68% 73% 100% 96% 10% 32%
GAIN SS Total Score is Correlated With Level Of Care Placement
Track Gap Between Prior and current Lifetime Problems to identify “under reporting” Track progress in reducing current (past month) symptoms) GAIN SS Can Also be Used for Monitoring 20 12+ mon.s ago (#1s) 2-12 Mon.s ago (#2s) 16 Past Month (#3s) Lifetime (#1,2,or 3) 11 12 10 10 9 9 8 8 3 4 2 2 0 Intake 3 6 9 12 15 18 21 24 Mon Mon Mon Mon Mon Mon Mon Mon Total Disorder Screener (TDScr) Monitor for Relapse
GAIN Quick (GQ) : Overview • Administration Time: 20-30 minutes (depending on severity and wether reasons for quiting module used) • Training Requirements: 1 day (train the trainer) plus certification within 1-2 months • Mode: Generally Staff Administered on Computer (can be done on paper or self administered with proctor) • Purpose: Designed for use in targeted populations to support brief intervention or referral for further assessment or behavioral intervention • Translation: English, with translations with us into Spanish by Chestnut and by collaborators being translated into French and Portuguese so far
GAIN Quick (GQ): Overview (Continued) • Scales: The GQ has total scale (99-symptoms) and 15 subscales (including more detailed versions of the GSS scales and subscales plus scales for service utilization, sources of psychosocial stress, and health problems). All scales focus on the past year only and it is primarily used to support motivational interviewing or for a one time assessment (though there is a shorter follow-up version). Lifeimt • Response Set: Breadth (past year symptom counts for behavior and lifetime for utilization) and Prevalence (past 90 days) • Interpretation: • Items can be used individually or to create specific diagnostic or treatment planning statements • Items can be summed into scales or indices for each behavior problem or and for recent service utilization overall • All scales, indices and selected individual items have interpretative cut-points to facilitate clinical interpretation and decision making • Reports: Narrative, tabular, graphical, validity and motivational interviewing reports built into web based GAIN ABS; Program level reports available in SPSS/Excel
GAIN Quick Profile of 4 Reclaiming Futures Sites(Range based on 0-24% / 25-74% / 75-100% of Symptoms) More detail within each area Risk Stress Health Source: Reclaiming Futures Chicago, IL, Dayton, OH, Portland, OR and Santa Cruz, CA sites (n=475). * Summary Measure
GAIN Quick Number of Problems Mod/Hi 97% endorsed one or more problems (69% 4 or more problems) Source: Reclaiming Futures Chicago, IL, Dayton, OH, Portland, OR and Santa Cruz, CA sites (n=475).
GAIN Quick (GQ): In Transition • Strengths: Length, Range of topics, Efficiently Categorize, Narrative reports to support screening, brief intervention, and referral to treatment • Problems: • Lacks scales to support analyses or outcomes related to change over time • Item response choices do not provide information about lifetime problems or problems that have occurred in finer gradations of time within the past year • Current Personal Feedback Report focuses only on substance use and does not address the other content areas of the GAIN-Q • Only about 60% of the items can be directly imported into the GAIN-I • Cut points do not map onto GAIN I or clinical criteria well • Plans for Version 3: • Keep focus on screening, brief intervention and referral to treatment • Subsume GSS and add similar screeners in other GAIN Q areas with recency response to address change and lifetime issues • Create a summary measure for days items to address change issues • Create reasons for change items in each area to support breif intervention, reducing number of items in substance use • Make all questions importable into full GAIN • Plans for Version 4: Add computer adaptive testing (CAT) component to get at more detailed diagnosis
GAIN Initial (GAIN-I): Overview • Administration Time: Core version 60-90 minutes/Full version 110-140 minutes (depending on severity and inclusion of GPRA module) • Training Requirements: 3.5 days (train the trainer) plus recommend formal certification program (administration certification within 3 months of training; local trainer certification within 6 months of training); Advanced clinical interpretation recommended for clinical supervisors • Mode: Generally Staff Administered on Computer (can be done on paper or self administered with proctor) • Purpose: Designed to provide a standardized biopsychosocial for people presenting to a substance abuse treatment using DSM-IV for diagnosis, ASAM for placement, and needing to meet common (CARF, COA, JCAHO, insurance, CDS/TEDS, Medicaid, CSAT, NIDA) requirements for assessment, diagnosis, placement, treatment planning, accreditation, performance/outcome monitoring, economic analysis, program planning and to support referral/communications with other systems • Translation: English, with translations with us into Spanish by Chestnut and by collaborators being translated into French and Portuguese so far
GAIN Initial (GAIN-I): Overview (Continued) • Scales: The GI has 9 sections (access to care, substance use, physical health, risk and protective behaviors, mental health, recovery environment, legal, vocational, and staff ratings) that include 103 long (alpha over .9) and short (alpha over .7) scales, summative indices, and over 3000 created variables to support clinical decision making and evaluation. It is also modularized to support customization • Response Set: Breadth (past year symptom counts for behavior and lifetime for utilization), Recency (48 hours, 3-7 days, 1-4 weeks, 2-3 months, 4-12 months, 1+ years, never) and Prevalence (past 90 days), patient and staff ratings • Interpretation: • Items can be used individually or to create specific diagnostic or treatment planning statements • Items can be summed into scales or indices for each behavior problem or type of service utilization • All scales, indices and selected individual items have interpretative cut-points to facilitate clinical interpretation and decision making • Reports: Narrative, tabular, validity and motivational interviewing reports built into web based GAIN ABS; New Narrative report include placement and treatment planning statements; Program level reports available in SPSS/Excel