Download
1 / 57
950 likes | 3.24k Views
DISEASES OF THE OPERATED STOMACH. PYLORUS. Distal muscular loop ; Proximal muscular loop. AGGRESSIVE FACTORS. hydrochloric acid pepsin reverse diffusion of ions of hydrogen products of lipid hyperoxidation. DEFENSE FACTORS. mucus and alkaline components of gastric juice

E N D
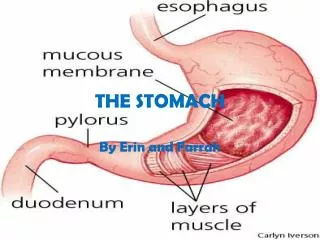
PYLORUS Distal muscular loop; Proximal muscular loop.
AGGRESSIVEFACTORS • hydrochloric acid • pepsin • reverse diffusion of ions of hydrogen • products of lipid hyperoxidation
DEFENSEFACTORS • mucus and alkaline components of gastric juice • property of epithelium of mucous tunic to permanent renewal • local blood flow of mucous tunic and submucous membrane
PATHOMORPHOLOGY • erosion • acute ulcers • chronic ulcers
CLASSIFICATION by Johnson (1965) • I – ulcers of small curvature (for 3 cm higher from a goalkeeper); • II– double localization of ulcers simultaneously in a stomach and duodenum; • III – ulcers of goalkeeper part of stomach (not farther as 3 cm from a goalkeeper)
CLINICAL MANAGEMENT • Pain • Vomiting • Heartburn • Belching
COMPLICATIONS • Penetration • Stenosis • Perforation • Bleeding • Malignization
DIAGNOSIS PROGRAM • 1. Anamnesis and physical examination. • 2. Endoscopy. • 3. X-Ray examination of stomach. • 4. Examination of gastric secretion by the method of aspiration of gastric contents. • 5. Gastric pH metry. • 6. Multiposition biopsy of edges of ulcer and mucous tunic of stomach. • 7. Gastric Dopplerography. • 8. Sonography of abdominal cavity organs. • 9. General and biochemical blood analysis. • 10. Coagulogram.
X-Ray examination THE DIRECT SIGNS: • symptom of “Haudek's niche” • ulcerous billow and convergence of folds of mucous tunic. INDIRECT SIGNS: • symptom of “forefinger” (circular spasm of muscles) • segmental hyperperistalsis, • pylorospasm, • delay of evacuation from a stomach • duodenogastric reflux • disturbance of function of cardial part (gastroesophageal reflux).
SURGICAL TREATMEN • at the relapse of ulcer after the course of conservative therapy; • in the cases when the relapses arise during supporting antiulcer therapy; • when an ulcer does not heal over during 1,5–2 months of intensive treatment, especially in families with “ulcerous anamnesis”; • ulcer with complications (perforation or bleeding); • at suspicion on malignization ulcers, in case of negative cytological analysis.
Classification of the postgastrectomy syndromes • Functional disturbance. • Dumping. • Hypoglycemic syndrome. • Postgastrectomy (agastric) asthenia. • Syndrome of small stomach. • Syndrome of afferent loop (functional origin). • Gastroesophageal reflux. • Alkaline reflux-gastritis. • Organic disturbances. • Pepticulcer of anastomosis. • Gastro-colon fistula. • Syndrome of afferent loop (mechanical variant). • Cicatricial deformation and narrowing of anastomosis. • Mistakes in the technique of operation. • Postgastrectomy accompanying diseases (pancreatitis, enterocolitis, hepatitis). • Mixed disturbances. • combination with dumping or postvagotomy diarrhea.
Distal resection of the stomach with saving of the perigastral vessels 1 3 2 4
Aiming resection of the ischemic segment of stomach in combination with SPV(by L.J. Kovalchuk) 3 2 межі резекції перехідного сегмента шлунка; формування гастро-гастроанастомозу: задня і передня губа; остаточний вигляд сформованого гастро-гастроанастомозу. 1
Proximal resection of the stomach межі резекції; завершений вигляд оперованого шлунка.
Proximalsubtotalresection of the somach схема операції; перерізання шлунка; перерізання абдомінального відділу стравоходу.
Gastrectomy(А – scheme; Б – end view) Esophago-jejunuanastomosis; Entero-entroanastomosis.
Depending on reasons and mechanisms of development of dumping syndrome there are different methods of the repeated reconstructive operations. All of them can be divided into four basic groups: • Operations which slow evacuation from stump of stomach. • Redoudenization. • Redoudenization with deceleration of evacuation from stump of stomach. • Operations on a thin bowel and its nerves.
Basic stages of reconstructive operations • disconnection of adhesions in an abdominal cavity, releasing of gastrointestinal and interintestinal anastomosis and stump of duodenum; • cutting or resection of efferent and afferent loops; • renewal of continuity of upper part of digestive tract.
Hypoglycemic syndromeThe attacks of weakness at a hypoglycemic syndrome arise up as a result of decline of content of sugar in a blood.
Distinguished easy, middle and heavy degrees of afferent loop syndrome
All operative methods of treatment of afferent loop syndrome can be divided into three groups: • Operations, that will liquidate the bends of afferent loop or shorten it. • Drainage operations. • Reconstructive operations.
CLASSIFICATION I. By etiology: А. True duodenal ulcer. B. Symptomatic ulcers. II. By passing of disease: 1. Acute (first exposed ulcer). 2. Chronic: a) with the rare exacerbation; b) with the annual exacerbation; c) with the frequent exacerbation (2 times per a year and more frequent).
CLASSIFICATION III. By the stages of disease: 1. Exacerbation. 2. Scarring: a) stage of “red” scar; b) stage of “white” scar. 3. Remission. IV. By localization: 1. Ulcers of bulb of duodenum. 2. Low postbulbar ulcers. 3. Combined ulcers of duodenum and stomach.
CLASSIFICATION V. By sizes: 1. Small ulcers up to 0,5 cm. 2. Middle — up 1,5 cm. 3. Large — up to 3 cm; 4. Giant ulcers over 3 cm. VI. By the presence of complications: 1. Bleeding. 2. Perforation. 3. Penetration. 4. Organic stenosis. 5. Periduodenitis. 6. Malignization.
CLINICAL MANAGEMENT • Pain • Vomiting • Heartburn • Belching
STENOSIS SYMPTOM OF “Haudek's niche”
DIAGNOSIS PROGRAM • 1. Anamnesis and physical examination. • 2. Endoscopy. • 3. X-Ray examination of stomach and duodenum. • 4. General and biochemical blood analysis. • 5. Coagulogram.
METHODS OF SURGICAL TREATMENT • organ-saving operations; • organ-sparing operations; • resection.