Download
1 / 43
760 likes | 1.72k Views
BIOLOGY OF ADDICTION:. What Neuroscience Has to Tell Us About Addiction as a Brain Disorder. Daniel P Logan, M.D., FACEP, ABAM Florida Recovery Center Addiction Medicine, Emergency Medicine Assistant Professor, Dept. of Psychiatry University of Florida College of Medicine.

E N D
BIOLOGY OF ADDICTION: What Neuroscience Has to Tell Us About Addiction as a Brain Disorder
Daniel P Logan, M.D., FACEP, ABAM Florida Recovery Center Addiction Medicine, Emergency Medicine Assistant Professor, Dept. of Psychiatry University of Florida College of Medicine
“Addiction is a primary, chronic disease of brain reward, motivation, memory and related circuitry. Dysfunction in these circuits leads to characteristic biological, psychological, social and spiritual manifestations…addiction often involves cycles of relapse and remission” ASAM Definition of ADDICTION
Brain Disorder • Matter of Will- “Disorder of Choice” • Bad Character • Self Medication Four Options to Explain Addiction
Moral Weakness or Stigma View weak willed bad irresponsible depressed immoral
Looks like weak willed – they should be able to stop if they put their mind to it • They caused it themselves • Your own experience with being able to stop drugs successfully • Consequences of use are immoral, sinful and bad • People should be aware that drugs are bad for them and should not have used them in the first place • Despite ‘good’ conventional medical, psychiatric and religious care, addicts get worse • It hurts others • Prejudice – your negative experience Why observations make you think it’s not a disease?
They seemed liked such normal people until they started using drugs • It tends to run in families • Not everyone who uses drugs becomes addicted • They use compulsively and can’t stop even with their best efforts • Has predictable symptoms – they get worse with time • Reasonable people would stop under those conditions • Some people like drugs and some don’t What observations provide evidence that it is a disease?
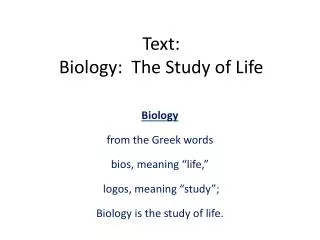
Decreased Brain Metabolism in Drug Abuse Patient High Control Cocaine Abuser Low ADDICTION IS A DISEASE OF THE BRAIN As other diseases, it affects tissue function Diseased Heart Healthy Heart Sources: From the laboratories of Drs. N. Volkow and H. Schelbert
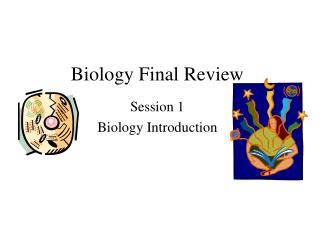
VTA Amphetamines Opiates THC PCP Ketamine Nicotine Alcohol benzodiazepines barbiturates Nucleus accumbens Dopamine Pathways
Dopamine(pleasure, learning) Serotonin(emotional stability) Norepinephrine (behavioral & physical activity) Pleasure (hunger/thirst/sexual), attention, organization of thought, muscle control and motor function Regulates mood, emotions, thought processes, sleep, and appetite Energy, motivation, attention span, alertness, pleasure, assertiveness, confidence, heart rate, blood pressure, etc. NTNormal Functions Glutamate and GABA
Inhibit Reuptake of Dopamine • Stimulate Dopamine transporter • Cocaine, Amphetamine, Methamphetamine, XTC • Modulate firing of Dopamine releasing cells by actions on GABA and Glutamate • Nicotine, alcohol, opiates, cannabis • Cocaine, Amphetamine, Methamphetamine, XTC How Drugs of Abuse Effect Dopamine
Drugs, Brains,and Behavior: The Science of Addiction; NIDA, March 2007
Adolescents • Risk taking • Novelty seeking • Responsive to peer pressure • Incomplete development of frontal regions involved in “executive function” Initiation of Addiction
The developing brain…….. What happens when you expose the developing brain to drugs during adolescence??
Earlier drinking more likely to result in alcohol dependence independent of family hx (Grant 1998) • Exposure of alcohol may indeed cause alterations in brain chemistry…. There are studies indicating heaving drinking during adolescence causes memory and neuropsychological changes (Brown, et al) • Alternative explanation that early use may simply be a marker for example high novelty seeking behavior which is associated with early use as well as a risk for alcohol dependence Adolescent Brain Changes
Animal studies show that early exposure to alcohol results in longer term problems such as cognitive and behavioral problems • Stress during adolescence maybe important factor in causing predisposition to etoh – adolescents perception of stress was associated with larger quantities of alcohol consumption • Remodeling of brain during adolescence – especially noted in the dopaminergic setting Adolescent Brain Changes
Genes either increase risk or are protective • Persistent drug use leads to gene transcription modification-part of neuro-plasticity • Htrlb receptor gene absence greater attraction to cocaine and alcohol • Curl receptor gene presence makes less responsive to morphine • ALDH*2 if two copies less likely to develop alcoholism Genetics
Twin studies in alcohol • Sway study of sons of alcoholics • If have one alcoholic parent 3-4 times increase risk of alcoholism Genetics
Homeostasis feedback-Allostasis “feed forward” • State of chronic deviation of regulatory system from normal i.e. homeostasis • “The New Normal” • “I don’t even get high anymore” • Brain adaptation to persistent drug exposure- NOT the same as tolerance ALLOSTASIS
Tolerance- defined by either of the following: • A need for markedly increased amounts of the substance to achieve intoxication or desired effect • markedly diminished effect with continued use of the same amount of the substance Tolerance
Withdrawal- the predictable constellation of signs and symptoms following the abrupt discontinuation of, or rapid decrease in, the consumption of a drug used consistently for a period of time. WITHDRAWAL
Decrease in Dopamine levels • Decrease in response to normally rewarding stimuli • Increase in “stress system” elevated CRF • Significant increase in anxiety and dysphoria Effects of Withdrawal
NOT just wanting or liking something • “I’m craving a Starbucks about now” • A MIDBRAIN (limbic system) process involving both memory and emotion • Similar to hunger and thirst • Previously neutral stimuli take on drug related significance Craving
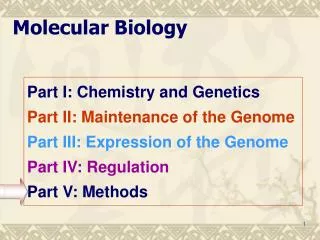
The Memory of Drugs Amygdalanot lit up Amygdalaactivated Frontof Brain Back of Brain Nature Video Cocaine Video
Re institution of drug taking • Persistence of dysregulation of reward system • Length of dysfunction related to drug and person • Triggered by: • Drug re exposure- may be other drug of abuse- need not be DOC • Emotional state • Stress RELAPSE
Nicotine appears to have very long lasting and strong persistence of midbrain sensitivity to nicotine re-exposure • Methamphetamine, XTC, bath salts- significant destruction of neurons both midbrain and cortex Differing Drug Effects
Daniel P Logan, M.D., FACEP, ABAM Florida Recovery Center Addiction Medicine, Emergency Medicine Assistant Professor, Dept. of Psychiatry University of Florida College of Medicine dlogan@ufl.edu 352.265.5549