Download
1 / 1
10 likes | 164 Views
Do We Need to Screen our IBD Patients for Depression: The Prevalence and Severity of Depression within a Typical DGH Cohort of IBD Patients. N. Swart 1 , D. Wellsted 1 , K. Lithgo 2 , T. Price 2 , M. W. Johnson 2.

E N D
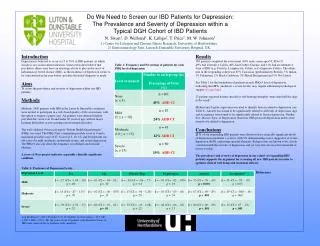
Do We Need to Screen our IBD Patients for Depression: The Prevalence and Severity of Depression within a Typical DGH Cohort of IBD Patients N. Swart1, D. Wellsted1, K. Lithgo2, T. Price2, M. W. Johnson2 1) Centre for Lifespan and Chronic Illness Research, University of Hertfordshire. 2) Gastroenterology Unit, Luton & Dunstable University Hospital, UK. Introduction Depression is believed to occur in 15 to 30% of IBD patients, in which suicide is not an uncommon ideation. Some researchers believe that psychiatric illness may have an aetiological role to play in the onset of inflammatory bowel disease (IBD), as the incidence of depression seems to be concentrated in the year before and after the initial diagnosis is made. Aims To assess the prevalence and severity of depression within our IBD patients. Methods Methods: 2400 patients with IBD in the Luton & Dunstable catchment were invited to participate in a web-based quality of life assessment, with the option to request a paper copy. All patients were deemed eligible provided they were over 18 and under 90 years of age, with no major learning difficulties or pre-existing serious mental disorders. The well validated 9-item self-report “Patient Health Questionnaire” (PHQ) was used. The PHQ-9 has a minimum possible score of 0 and a maximum possible score of 27. Scores of 5, 10, 15, and 20 represent cut-off scores for mild, moderate, moderately severe, and severe depression. The PHQ-9 also ask about the frequency of self-harm and suicidal ideation. A score of 10 or greater indicates a possibly clinically significant condition. Results 360 patients completed the assessment (44% male; mean age=53, SD=17). 49% had Ulcerative Colitis, 40% had Crohn’s Disease, and 11% had an alternative form of IBD (e.g. Proctitis, Lymphocytic Colitis, or Collagenous Colitis). The ethnic mix in the responding cohort was 87% Caucasian (predominately British), 3% Indian, 3% Pakinstani, 2% Black Caribbean, 2% Mixed Background and 3% Not Stated. See Table 1 for the breakdown of patients in each PHQ-9 level of depression, indicating that 21% (moderate + severe levels) may require additional psychological support of some kind. 23 patients reported having suicidal or self-harming thoughts “more than half the days in the week”. Multinomial logistic regression was used to identify factors related to depression (see Table 2). Anxiety was found to be significantly related to all levels of depression. Age and Acceptance were found to be significantly related to Severe depression. Neither Sex, Disease Type, or Deprivation (based on OBS postcode deprivation index) were found to be related to depression. Conclusions 21% of our responding IBD patients were shown to have clinically significant levels of depression (moderate + severe), with 5% demonstrating scores suggestive of severe depression (6.3% expressing suicidal ideation). Relapse rates are known to be closely correlated with the severity of depression, and yet very few are on active treatment or review for this. The prevalence and severity of depression in our cohort of responding IBD patients supports the argument for screening all new IBD patients in order to optimise clinical well-being and treatment efficacy. Table 1: Frequency and Percentage of patients for each PHQ level of depression Table 2: Predictors of Depression Levels References Log likelihood = -229.1; Pseudo r2 = 0.43; Number of observations = 317; AIC = 500.1; BIC = 579.1. Nb. the scores of the 38 patients with alternative forms of IBD were removed due to problems with model fit.