Download

1 / 28
280 likes | 559 Views
Canine Mammary Tumors تومورهای پستانی سگ ها. Dr.Doosti. مقدمه :. تومورهای پستانی شایعترین سرطان در سگهای ماده است. تقریباً 80 درصد تومورهای پستانی در ماده سگهای با سن بیش از هفت سال تشخیص داده میشوند. در حدود 30 درصد این موارد کارسینومای بدخیم است. این تومورها ممکن است تکی یا چندتایی باشند.

E N D
مقدمه : تومورهای پستانی شایعترین سرطان در سگهای ماده است. تقریباً 80 درصد تومورهای پستانی در ماده سگهای با سن بیش از هفت سال تشخیص داده میشوند. در حدود 30 درصد این موارد کارسینومای بدخیم است. این تومورها ممکن است تکی یا چندتایی باشند.
نوع تومورها : • بر اساس اعلام سازمان جهانی بهداشت ، از نظر بافت شناختی تومورهای پستانی به 4 دسته تقسیم میشوند. تومورهای بدخیم ، تومورهای خوش خیم ، تومورهای بدون طبقه بندی و هایپرپلازی پستان • شایعترین نوع تومورها تومورهای میکس خوش خیم ، آدنوما و آدنوکارسینوما است. تومورهای مختلط خوش خیم متشکل از تومورهای اپی تلیال و تومورهای مزانشیمال هستند که می توانند سلولهای استخوانی ، غضروف یا فیبروز داشته باشند. • آدنوما و آدنوکارسینوما به انواع مختلفی تقسیم میشوند. کارسینومای غیرمنتشر ، کارسینومای کمپلکس ، کارسینومای ساده و کارسینومای آناپلاستیک ساده از این جمله اند.
علل و عوامل خطرساز : • علت بروز تومور پستانی هنوز دقیقاً معلوم نیست ، با این حال عوامل متعددی در بروز آن دخالت دارند. هورمونهایی مثل استروژن و پروژسترون در این زمینه مؤثرند. این مسئله را می توان اینطور توجیه نمود که عمل OHE احتمال ابتلا به تومور پستانی را کاهش میدهد. اگر ماده سگ قبل از اولین فحلی عقیم شود احتمال بروز تومور پستانی به کمتر از یک دصد محدود میشود
علل و عوامل خطرساز : • اگر بین اولین تا سومین فحلی اینکار انجام گیرد شانس ابتلا 8 تا 26 به ترتیب قبل از دومین و سومین فحلی خواهد بود. عقیم کردن حیوان بعد از سومین فحلی را خیلی مؤثر در جلوگیری از ابتلا به تومورهای پستانی نباید دانست. چاقی هم از جمله عوامل خطرساز بروز تومور پستانی است. استعداد ارثی که در طب انسانی به عنوان یک عامل خطرساز اثبات شده است در دامپزشکی هنوز در مراحل تحقیق قرار دارد.
علائم بالینی : • تومورهای پستانی ممکن است در اندازه های متفاوتی بروز نمایند. تکی یا چندتایی ، نرم یا سفت باشند. به طور کلی تا پیشرفت محسوس تومور صاحب حیوان در اغلب موارد قادر به تشخیص توده نخواهد بود.
تشخیص : • معاینه بالینی و ملامسه اولین اقدام در جهت تشخیص است. اغلب موارد تومور در جفت عقبی پستان بروز میکند. شمارش کامل خون و بیوشیمی خون هم باید انجام پذیرد. تهیه رادیوگراف های جانبی چپ و راست و VD سینه و دو نمای جانبی و VD شکم در تشخیص متاستاز فوق العاده مفید خواهد بود. اگر به متاستاز شکمی مشکوک باشیم می توان از سونوگرافی هم بهره برد. • بیوپسی هم از تومور می تواند در پاتولوژی مشخص کننده نوع آن باشد. • بر اساس سایز تومور ، متاستاز به عقده های لنفاوی و متاستاز به سایر اندامها بیماری را به 5 مرحله تقسیم میکنند که هر چه به مرحله پنجم نزدیک شویم پیش آگهی درمان ضعیف تر خواهد بود.
تشخیص : • 5 مرحله به شرح زیر است : • 1 - قطر تومور کمتر از سه سانتی متر است. و متاستازی وجود ندارد. • 2 - قطر تومور بین سه تا پنج سانتی متر است و متاستازی وجود ندارد. • 3 - قطر تومور بیش از پنج سانتی متر است و متاستازی وجود ندارد. • 4 - صرفنظر از قطر تومور ، متاستاز به عقده های لنفاوی رخ داده است. • 5 - صرفنظر از قطر تومور و متاستاز به عقده های لنفاوی ، اندامهای دیگر بدن هم دچار متاستاز شده اند.
Etiopathology • Endogenous estrogen and progesterone are regarded • as having a central role in the etiology of MGTs. • Estrogen and progesterone receptors (ERs, PRs) are • found in 50% of malignant and 70% of benign MGTs • as well as in normal mammary gland tissue.9,10 This • is consistent with the concept that deviation from • normal control mechanisms develops progressively in • malignant MGTs.11,12 Tumors that do not have hormone • receptors have a more aggressive behavior and are less • differentiated than those that express the receptors.13 • Moreover, the presence of steroid receptors is infrequent • in metastases, which may indicate an autonomous • pattern of growth.13 In humans, tumors rich in ERs • alone or ERs and PRs regress after ablative endocrine • therapy but tumors lacking receptors do not respond • and are associated with a poorer prognosis.14
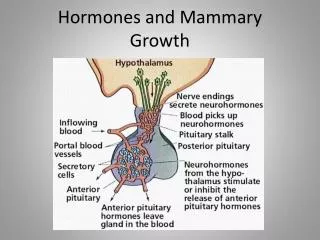
Etiopathology • Other growth factors could play a role in the • development of normal and neoplastic mammary tissues, • including epidermal growth factor (EGF), transforming • growth factors (TGFs),15,16 and parathyroid hormone– • related protein.17 EGF and TGFs are associated with • the presence of ERs and PRs in MGTs; in malignant • tumors, a direct correlation was observed between EGF • and ER expression.18 • The role of mammotrophichypophyseal hormones in • mammary tumorigenesis is still controversial. Prolactin • and growth hormone (GH) physiologically stimulate • tubuloalveolar development, mammary differentiation, • and lactogenesis. However, basal GH and prolactin levels • were found to be similar in tumor-bearing and agematched • bitches in previous studies.19,20
Etiopathology • Other studies suggested that high prolactin serum concentrations • could increase the appearance of preneoplastic • lesions.21,22 Progestin-induced GH excess could influence • MGT development,16,23 which may occur by the • stimulated proliferation of susceptible and transformed • mammary epithelial cells.24 Receptors for prolactin,12 • glucocorticoids,25 and dihydrotestosterone26 have also • been found in MGTs.
Etiopathology • The risk of MGT development is approximately • 0.5% for bitches spayed prior to their first estrus, 8% • for those spayed after the first estrous cycle, and 26% • for those spayed after the second cycle. After that time, • the protective effect is minimal,27,28 although the risk • of developing benign tumors may still be reduced.9 • However, the long interval between ovariectomy and • tumor development may be associated with a decline • in ER expression and a decreased benefit from ovarian • hormone ablation or antiestrogen therapy. Age at peak • incidence for MGTs is the same for neutered and intact • bitches.7
Etiopathology • Administration of long-acting progestins for estrus • prevention has been found to be associated with benign • MGTs in bitches.16,21,23 Estrogen treatments used for • pregnancy termination also increase the risk for • MGTs.16,21 No clear relationship between MGTs and • characteristics of the estrous cycle or parity has been • demonstrated.3,16 It has been suggested that frequent • pseudopregnancy episodes could increase the appearance • of preneoplastic lesions.21,22 Obesity and a high-fat diet • at a young age have also been associated with a poorer • prognosis and increased risk for MGTs, respectively.29,30
HISTOPATHOLOGY • Histologic classification is difficult due to the diversity • of presentations, but an acceptable scheme was proposed by Misdorp and colleagues.31 Approximately 50% • to 60% of canine MGTs are benign, and most of these • are fibroadenomas. The other 40% to 50% of MGTs • are malignant, and 50% of these may metastasize.1 • Benign tumors can be mixed MGTs (having epithelial • and mesenchymal components), adenomas, or benign • mesenchymal tumors.
HISTOPATHOLOGY • Adenocarcinomas are the • most frequent malignant MGT, but sarcomas and malignant • mixed MGTs also occur. Sarcomas represent • approximately 5% of malignant MGTs and have a • higher risk of metastasis than carcinomas.32 Inflammatory • carcinomas are poorly differentiated with an extensive • inflammatory infiltrate. These tumors often • cause marked edema and ulceration of the mammary • chain and hindlimbs. Disseminated intravascular coagulation • is common in dogs with this tumor.33
TREATMENT • The treatment of choice for MGTs is surgical excision. • Techniques include lumpectomy, simple mastectomy, • unilateral mastectomy, bilateral mastectomy, and • radical mastectomy.10 The pros and cons of radical versus • local excision have been extensively debated. Selection • of the technique depends on tumor size, number • of mammary glands affected, location, fixation to the • underlying tissue, and the patient’s medical status. • Most data suggest that the method of removal is not as • important for prognosis as is obtaining microscopically • clean margins,34,35 and no prospective clinical trial has • shown an improved survival for patients undergoing • radical mastectomy.36 Lymph node excision is imperative • if cytology reveals tumor cells.
TREATMENT • A recent study indicated that ovariectomy performed • concurrently with MGT removal prolongs survival time • not only in patients with benign tumors but also in • those with malignant MGTs.37 In bitches spayed within • 2 years prior to or concomitant with surgery, survival • was 45% longer than in those that were not. Therefore, • neutering all bitches at the time of MGT removal • should be considered.
REFERENCES • 1. Moulton JE: Tumors of the mammary gland, in Moulton JE • (ed): Tumours in Domestic Animals, ed 3. Berkeley, University • of California Press, 1990, pp 518–552. • 2. Cotchin F: Further observations on neoplasias in dogs with • particular reference to site of origin and malignancy. Br Vet J • 110:218, 1954. • 3. Misdorp W: Canine mammary tumors: Protective effect of • late ovariectomy and stimulating effects of progestins. Vet Q • 10:26–33, 1988. • 4. Perez A, Peña L, Del Castillo N, Nieto AI: Factors influencing • the incidence and prognosis of canine mammary tumours. • J Small AnimPract 41:287–291, 2000. • 5. O’Keefe D: Tumors of the genital system and mammary • glands, in Ettinger SJ (ed): Textbook of Veterinary Internal • Medicine, ed 3. Philadelphia, WB Saunders Co, 1995, pp • 1699–1704.
Thanks for your Attention The End