Download
1 / 21
220 likes | 405 Views
Improving Referring Provider Communication. Performance Improvement Leadership Development Program Center for Health Care Quality University of Missouri – Columbia. Team. Provider Champion/Coach/Facilitator Kevin Dellsperger, MD Kristin Hahn-Cover, MD Team Members

E N D
Improving Referring Provider Communication Performance Improvement Leadership Development Program Center for Health Care Quality University of Missouri – Columbia
Team • Provider Champion/Coach/Facilitator • Kevin Dellsperger, MD • Kristin Hahn-Cover, MD • Team Members • Cindy Feutz, RN, Clinical Nurse Specialist (Cardiology) • Jordan Magdits, Assistant Manager (Admissions) • Sherry Rickard, RN , Case Manager (Family & Community Medicine) • Tracy Riecke, RN, Case Manager (Orthopaedic Surgery) • Krista Romanetto, Supervisor (Medical Records) • Matt Wilp, Manager (Provider Relations) • Resources • Candice Monnig (Cardiology) – Joanne Burns (IT) • Colette Nolin (Admissions) – John Guyton (IT) • Becky Morton (Medical Records) – Scott Barger (IT) • Carol Toliver (Finance) – Doug Garrison (Admissions) • Executive Sponsor – Marty McCormick, Director, Planning
Focus Area & Aim • Problem • Over the past 12 years, communication has consistently ranked as the leading cause of dissatisfaction for referring/primary care providers. • Timeliness of communication • Quality of communication • Poor communication has a negative impact on: • Patient safety and outcomes • Referral volumes • Aim Statement - we aim to improve communication within one business day of discharge to external referring and primary care providers whose patients receive in-bed services at University Hospital by increasing successful transmission of discharge documentation from 28% to 100% by April 1, 2011.
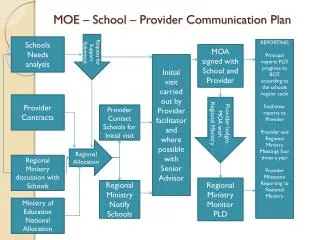
Timeline • August 2010 – Project Began • September - November 2010 – Diagnostic Journey • November 2010 – Interventions chosen – reintroduce scripting & pursue automation • November 2010 – Admissions/Registration reinforces scripting to staff • December 2010 – Dr. Hahn-Cover presents recommended changes to Executive Committee; approved by Executive Committee • December 2010 - February 2011 – Rapid Cycle PDSA • February 2011 – Pilot process of faxing Depart Summary to referring and primary care provider • February 2011 – Dr. Hahn-Cover presents updated recommendations to Executive Committee
Relationship to Strategic Goals • Service Column of Excellence • FY15 • Goal - To become the provider of choice through exceptional patient- and family-centered care • Targets/measures - referring provider satisfaction mean score of 80 • FY11 • Objective/tactics • Develop and implement a process to provide communication within one to two business days of discharge to the referring/primary care provider • Develop a succinct discharge summary that meets the needs of referring providers and improves coordination of care and outcomes • Targets/measures • Implementation of inpatient discharge notification process; 80% of external referring physicians receive a phone call within two business days of patient discharge • Development of discharge summary
Stakeholders • External referring/primary care providers • Patients • Patient care staff (e.g. physicians, fellows, residents, nurses, case managers, discharge planners, etc.) • Revenue cycle • Information technology • Provider relations
Driver Diagram III - 3 IIII - 4 II - 2 I - 1 II - 2 III - 3
Interventions Chosen • Immediate/Short-term • Reinforce scripting for registration/admissions staff to better clarify what a referring and primary care provider is to patients • Fax Depart Summary to referring and primary care provider by next business day after patient discharge • Long-term • Develop an automated process to send out all communication (admission note, operative notes, succinct discharge summary, clinician summary) within timeframe outlined in Medical Staff Bylaws • Roll out this process to all areas at University Hospital as well as all other MUHC facilities (WCH, MUPC, EFCC, clinics, etc.)
Measurement • Measure the percentage of external referring and primary care providers who are sent follow-up communication • Key measures for this process include: • Primary care provider complete • Referring provider complete • Proportion of providers that are external • Time interval between date of discharge and date documentation is faxed • Fax sent successfully
Baseline Data • 429 discharges measured in November 2010
Baseline Data • 63 External Referring Providers
Baseline Data • 139 discharges measured in January 2011 • 94 external referring or primary care providers listed • 28% (26 of the 94) of patients’ providers receive follow-up communication • Low percentage due to current UH process of only sending documentation to referring provider
Pilot Data – February 2011 156 Patients Discharged 61 Internal Referring Provider or PCP or Self 95 Patients with External Referring Provider or PCP 12 Patients Depart Summary Not Required 4 Patients Expired 79 Patients with External Providers 75 Providers Received Documentation (95%)
Process & Outcome Indicators • Process Indicators • Registration Services to include the completion of referring and primary care provider field into daily QA process • Medical Records to include QA process of recording verification of faxes sent to referring and primary care providers • Outcome Indicators • Continuity of care for patient safety and decrease in avoidable readmissions • number of referring and primary care providers receiving follow-up communication • Referring physician satisfaction • Referrals volumes
Benefits • Quality – improving communication to referring physicians will enhance the coordination of care and patient outcomes and prevent avoidable readmissions • Service - increased referring physician and patient satisfaction • People – increased physician satisfaction and retention • Growth - the Advisory Board states that physicians are the most important driver of market share: • 35% - primary physician is affiliated with hospital • 31% - hospital provides specialized services • 31% - advice/referral from physician • 21% - hospital is up-to-date with medical advances • Finance • Reimbursement increasingly being tied to quality of care and outcomes • FY10 net revenue/adjusted case YTD (excl. FRA and retail pharmacy revenue) • University Hospital - $13,712 • CRH (now W&CH) - $ 13,152
Anticipated ROI • MUHC has aggressive growth and financial targets • FY10 actual discharges were 21,279 and the FY11 budgeted discharges are 23,064. This is an 8.4% (1,785) increase in discharges • The FY11 budgeted change in net assets is $30.0 million • Assuming average net revenue per adjusted case of $13,500, MUHC could experience the following improvement in performance: • 2% (425) increase in discharges would result in an additional $6.5 million in net revenue • 6.5% (1,383) increase in discharges would result in an additional $18.6 million in net revenue • 10% (2,127) increase in discharges would result in an additional $28.7 million in net revenue • Medical Records estimates a saving of at least 2 hours of employee time per day when implementing the process of faxing Depart Summaries
Lessons Learned • The situation is more complex than anticipated and requires collaboration on the part of many • Patients need clarification of what a primary care physician is • Residents and attendings have ownership in completing discharge summaries and signing off in a timely manner • A clear/concise discharge summary or Depart Summary for referring and primary care providers needs to be developed • The provider dictionaries need to be combined and maintained and IT systems need to interface • The process needs to be centralized to improve quality and reduce inefficiencies • Both the referring physician and the primary care physician should receive communication • The reason that documentation was sent to only referring providers was because years ago the referring provider field was the most filled out field • Sometimes change to hospital policy is needed and can be time consuming
Summary • We have only taken on a very small part in improving overall communication to referring providers • In an ideal world an automated process is the best answer, but the bottom line is it can only be as good as the data that is available to it; the goal is to achieve automation by July 2012 • With a major emphasis on outcomes and avoidable readmissions, improved coordination of care through communication to referring and primary care providers is essential • Improving quality of care and outcomes and increasing the satisfaction of our referring providers will assist in achieving the volume growth needed to support MUHC’s strategic financial plan • We feel our biggest accomplishment so far was discovering that primary care providers were not receiving communication and mirroring our current process to get communication to them