Skin Anatomy and Disorders Overview for Medical Professionals
Explore the layers of the skin, sensory nerves, sweat glands, melanoma, and more in this comprehensive guide. Learn about different types of skin cancers, benign cysts, and scar tissue management. This resource aims to provide valuable insights into skin health and conditions.


Skin Anatomy and Disorders Overview for Medical Professionals
E N D
Presentation Transcript
1. SKIN Western Reserve Care System
Northside Medical Center
Department of Surgery
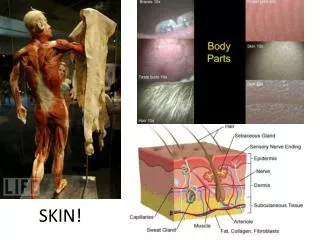
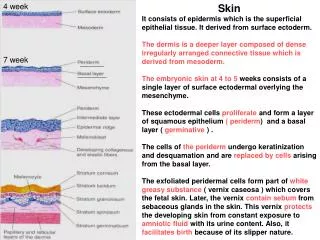
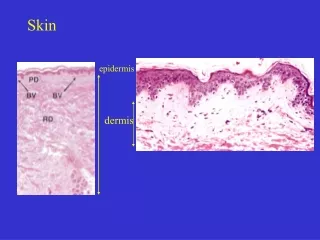
2. Anatomy Layers of the Skin:
Epidermis
Keratinocytes
Melanocytes
Dermis
Skin Appendages
Hair Follicles
Sweat Glands
Eccrine or merocrine sweat glands
Apocrine sweat glands
Sebaceous glands
3. Sensory Nerves Pacinian Corpuscles � pressure
Ruffini�s Endings
� warmth
Krause�s end bulbs
� cold
Meissner�s Corpuscles
� tactile sense
4. Sweat Glands Exocrine Glands � aqueous sweat (thermal regulation, hypotonic usually)
Apocrine Glands � milky sweat, highest concentration in palms and soles
5. Langerhans Cells Act as antigen presenting cells
Originate from bone marrow
Act in role as hypersensitivity reaction (Type IV)
6. Misc. Facts Lipid soluble Drugs have increased skin absorption
Type I collagen- gives tensile strength and makes up 70% of dermis
Tension is provided by collagen in skin
Elasticity ability of regain shape
Cushings�s Striae � loss of both tensile strenght and elasticity.
7. Pressure Ulcers
8. Example Stage IV Ulcer
9. Melanoma Risk Factors:
1) dysplastic, atypical or lg congenital nevi
2) Familial BK mole syndrome
3) Xeroderma Pigmentosum
Most common site of melanoma � back in men, legs in women
10. Melanoma Manifestations
11. Melanoma Continued Worse prognosis for men, ulcerated lesions, occular or mucosal lesions
Originates form neural crest cells in basal layer of the epidermis
Lung is most common location of distant metastases
Small bowel is most common overall location of metastases
14. Basal Cell Carcinoma MC malignancy in US, 4x MC than squamous
Pearly appearance, rolled borders
Peripheral palisading of nuclei and stromal retraction
Ulcerative, no metastases, deep invasion
Morpheaform type is most aggressive, has collagenase production, Tx w/.3-.5cm margins
15. Basal Cell Carcinoma
17. Squamous Cell Carcinoma Risk Factors � actinic keratoses, zeroderma pigmentosum, bowen�s disease, atrophic epidermitis, arsenic, coal tar, nitrates, HPV, fair skin, XRT exposure
Tx: .5-1.0cm margins for low risk
Reginal adenectomy for positive nodes
Mohs Surgery � margin mapping using conservative slicles, never used for melanoma, best for facial lesions
18. Squamous Cell Carcinoma
19. Kaposi�s Sarcoma Vascular sarcoma
Can involves, skin, mucus membranes of GI tract
Associated with AIDS/HIV
Tx XRT of intralesional vinblastine for lcoal disease, Sx for intestinal hemorrage
20. Xanthomas Yellow lesions, associated with fatty deposition. Contain histocytes. Tx excision.
21. Verruca Vulgaris HPV viral origin
Tx liquid nitrogen
Gardacil Vaccine protects against several varities of skin as well as cervical HPV
22. Neuromas Associated with NF1 & NF2. Look for caf� au lait spots or axillary freckling for dx.
23. Keratoses Actinic Keratosis � premalignant, sun damamged ares, Bx if suspicious
Seborrheic Keratosis � no premalignant, trunk of elderly
Arsenical keratosis � assoicated with squamous cell carcinoma
24. Benign Cysts Epidermal Inclusion Cysts
MC, mature epidermis with creamy keratin material
Trichilemmal Cyst
In scalp, no epidermis
Ganglion Cyst
Over tendons, usually on wrist, filled with collagenous material
25. Benign Cysts Continued Pilonidal Cyst
Congenital coccygeal sinus with ingrown hair, excise the wall
26. Keloids Autosomal Dominant
Collagen goes beyond original scar
Tx: XRT, steroids, silicone, pressure garments
27. Hypertrophic Scar Tissue Predisposition � dark skin, flexor surfaces of upper torso
Collagen stays within confines of scar
Often occurs in burn tissue
Tx: steroids, silicone, pressure garments