Babesia microti
Babesia microti. Jessica Grams & Jennifer Wimpfheimer. Outline…. Taxonomy Babesiosis Morphology Geographic Distribution Hosts Life Cycle Pathogenesis/Clinical Signs & Symptoms Host Immune Response Diagnosis Treatment Public Health Concerns Crossword puzzle. Taxonomy.

Babesia microti
E N D
Presentation Transcript
Babesia microti Jessica Grams & Jennifer Wimpfheimer
Outline… • Taxonomy • Babesiosis • Morphology • Geographic Distribution • Hosts • Life Cycle • Pathogenesis/Clinical Signs & Symptoms • Host Immune Response • Diagnosis • Treatment • Public Health Concerns • Crossword puzzle
Taxonomy • Kingdom: Protista • Phylum: Apicomplexa • Class: Aconidasida • Order: Piroplasmida • Family: Babesiidae • Babesiamicroti
Babesiosis • Prior to 1969 Babesia infections were rare and limited to B. divergens (a cattle parasite) and some others species that were parasitic in rodents. • It was only seen in splenectomized patientswho had disabled immune systems as a result of the splenectomy. • 1969, Nantucket Island, Mass: 1st human Babesia infection in a non-splenectomized patient. • Hundreds of cases have been reported since.
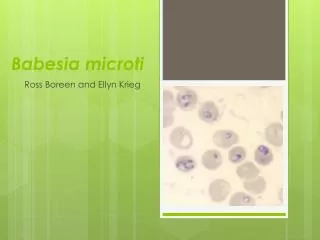
Morphology • Easily misdiagnosed as Plasmodium in areas high in Malaria prevalence due to its “ring shape” • Variation in shape and size • Do not produce pigment Intraerythrocytic Babesiamicroti
Geographic Distribution • Worldwide • Europe: B.divergens, most common • United States: B. microti, most common in NE and MW portions • WA-1 strain recently found on west coast * May not be as prevalent in malaria-endemic countries*
Hosts • Definitive host: Humans or Deer tick • Vector: Ixodes scapularis (Deer tick) • Intermediate host: White-footed mouse and other rodents and Deer • When the deer or mouse pop. increases, the tick pop. does too.
Life Cycle • Babesia infected tick introduces sporozoites into the mouse host. • Sporozoites enter erythrocytes and undergo asexual reproduction (budding). • In the blood, parasites undergo male and female differentiation (micro- and macrogametes are formed). • The deer tick (definitive host) takes a blood meal ingesting gametes, which can now undergo fertilization within the gut, 5. resulting in sporozoite formation. Spread to salivary glands.
Life Cycle Cont’d… 6. During a blood meal, the tick infects the human host. Inoculation occurs by a tick larva, nymph or adult. • Sporozoites invade erythrocytes and a trophozoite differentiates, replicating asexually by budding: responsible for the clinical manifestations. This forms 2-4 merozoites which eventually reinvade other RBCs. • Humans are for all practical purposes “dead-end” hosts, because subsequent transmission after the tick feeds on a human is unlikely. Human to human transmission is well recognized to occur through blood transfusions. Babesia can be transmitted in utero.
Pathogenesis (Signs & Symptoms) • 1-4 weeks (can last several weeks): fever, chills, headache, nausea, vomiting, and/or muscle aches (myalgia), hemolytic anemia, jaundice and splenomegaly. • May be mild in otherwise healthy people • May be asymptomatic • Severe form of Babesiosis may be life-threatening if untreated (usually people who have been splenectomized, the elderly, or who have impaired immune systems).
Host Immune Response • Mice develop immunity • CD4 T cells are partially responsible for resolution of primary infection and protection against re-infection. • Influx in IgG due to the infection being in the blood
Diagnosis • Microscopic examination: thick and thin blood smears stained with Giesma • Antibody detection: detects even low levels of parasitic invasion • Indirect fluorescent antibody test (IFA) detects antibodies (IgM & IgG) of patients with B. microti infection • Recommended only if low levels of parasitemia or blood smear is inconclusive • Diagnosis can be derived from molecular techniques, such as PCR • Valuable in investigations of new Babesia species
Treatment • Clindamycin*: antibiotic with little or no side effects • Quinine or Atovaquone*: antiparasitic • Azithromycin*: antibiotic, some side effects • Clindamycin combined with Quinine is treatment of choice *FDA approved, but considered investigational
Public Health Concerns • Avoidance of endemic areas May-September • Clothing that covers lower body and light colored • Tuck pants into boots/shoes • Repellent that contains Diethyltoluamide (DEET) should be applied regularly • Inspect pets • Avoid tall grass and brush • Examine skin thoroughly and carefully remove ticks if found • Avoid accepting blood donations from those with a history of tick bites
In conclusion, be aware of your surroundings, especially in areas with high deer tick populations.