Download
1 / 24

E N D
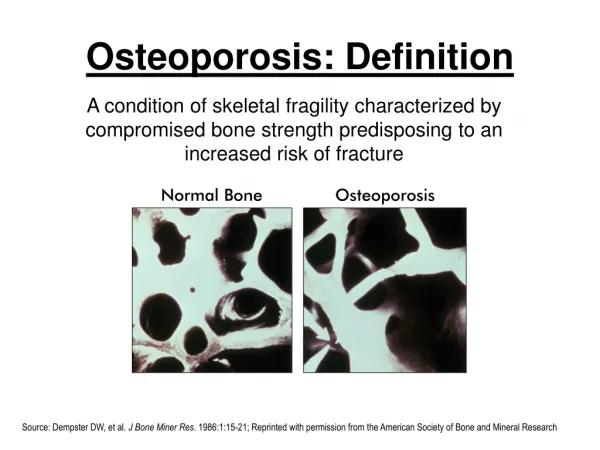
Osteoporosis: Definition A condition of skeletal fragility characterized by compromised bone strength predisposing to an increased risk of fracture Normal Bone Osteoporosis NIH Consensus Development Conference Statement, on Osteoporosis Prevention, Diagnosis, and Therapy, 2000. Source: Dempster DW, et al. J Bone Miner Res. 1986:1:15-21; Reprinted with permission from the American Society of Bone and Mineral Research
513,000 Heart Attack Frequency of CommonMedical Events in Women 2,000,000 * 1,500,000 1,500,000 250,000hip 250,000forearm Annual incidence of common diseases 1,000,000 250,000 other sites ** 500,000 † 228,000 750,000 vertebral ‡ 184,300 0 Osteoporotic Stroke Breast Cancer Fractures * annual incidence all ages ** annual estimate women 29+ † annual estimate women 30+ ‡ 1996 new cases, women all ages 1. Riggs, B.L., and Melton, L.J. III, Bone 17(5)(Suppl.):505S-511S, 1995 2. Heart and Stroke Facts: 1996 Statistical Supplement, American Heart Association 3. Cancer Facts & Figures—1996, American Cancer Society
Prevalence • Osteoporosis is a health threat for an estimated 44 million Americans. • Of that 44 million : • 10 million individuals already have the disease • 80% of these are women • 34 million more are estimated to have low bone mass and increased risk for osteoporosis. • Osteoporosis affect people of all ethnic backgrounds. • While osteoporosis is often thought of as an older person's disease, it can strike at any age.
Cost • The estimated national direct expenditures for osteoporotic hip fractures was $18 billion dollars in 2002. • Office visits have increased five-fold (from 1.3 to 6.3 million) in the past 10 years. • In 2001, about 315,000 Americans age 45 and over were admitted to hospitals with hip fractures. Osteoporosis is highly preventable. However, if the toll of osteoporosis is to be reduced, the commitment to osteoporosis research must be significantly increased. It is reasonable to project that with increased research, the future for definitive treatment and prevention of osteoporosis is very bright.
Fractures • An average of 24 percent of hip fracture patients aged 50 and over die in the year following their fracture. • Only 15 percent of hip fracture patients can walk across a room unaided 6 months later. • Hip fractures AND vertebral fractures are linked with an increased risk of death. • One in five hip fracture patients ends up in a nursing home, a situation that participants in one study described as less desirable than death.
Fractures • Hip fracture risk is increasing most rapidly among Hispanic women. • Women with a hip fracture are at a four-fold greater risk of a second one. • Osteoporotic fractures lower a patient’s quality of life. One in two women and one in four men over age 50 will have an osteoporosis-related fracture in her/his remaining lifetime. Annually, 1.5 million osteoporotic fractures occur: 300,000 hip fractures 700,000 vertebral fractures 250,000 wrist fractures 300,000 fractures elsewhere
Estimates of Osteoporosis in Women >50 yr old • Non-Hispanic white and Asian women: • 20% have osteoporosis; 52% have low bone mass. • Non-Hispanic black women: • 5% have osteoporosis; 35% have low bone mass • Hispanic women: • 10% have osteoporosis; 49% have low bone mass. • Osteoporosis is under-recognized and under-treated not only in Caucasian women, but in African-American women as well.
Shrinking is NOT an Inevitability of Aging and IS NOT normal!! • White women ≥65 year old have twice the fracture incidence versus African-American women. • Women have a hip fracture rate two to three times higher than men. • A woman's risk of hip fracture is equal to her combined risk of breast, uterine and ovarian cancer. Osteoporosis and Women Bone loss during breastfeeding? Bone density can be temporarily lost during breastfeeding. Several studies have shown that recovering full bone density occurs within six months after weaning.
Etiology • Rheumatologic disorders • rheumatoid arthritis, • ankylosing spondylitis INHERITED DISORDERS • Marfan syndrome • hemochromatosis • Hypophosphatasia • epidermolysis bullosa • homocystinuria • porphyria • Menkes' syndrome • osteogenesis imperfecta • Ehlers-Danlos syndrome • glycogen storage diseases OTHER DISORDERS • immobilization, • pregnancy and lactation • scoliosis • chronic obstructive pulmonary disease • amyloidosis • use of glucocorticoids • Iatrogenic osteoporosis caused by the therapeutic
Etiology • Nutritional and gastrointestinal disorders • malnutrition, • parenteral nutrition, • malabsorption syndromes, • gastrectomy, • severe liver disease (especially biliary cirrhosis), • pernicious anemia. • Endocrine disorders • Cushing's syndrome, • hyperparathyroidism • thyrotoxicosis, • insulin-dependent diabetes mellitus, • acromegaly, • adrenal insufficiency • Hematologic disorders/malignancy • multiple myeloma, • lymphoma and leukemia, • mastocytosis, • hemophilia, • thalassemia. • Hypogonadal states • Turner syndrome, • Klinefelter syndrome, • Kallmann Syndrome, • anorexia nervosa, • hypothalamic amenorrhea, • hyperprolactinemia.
Symptoms • Osteoporosis, the "silent disease," has bone loss without symptoms. • Onset only occurs with sudden strains, bumps, or fall causes a fracture or a vertebra to collapse. • Collapsed vertebrae may initially be felt or seen in the form of severe back pain, loss of height, or spinal deformities such as kyphosis or stooped posture.
1.4 Mean–2 SDConsider preventive interventionConsider therapeutic intervention 1.3 1.2 1.1 BMD 1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 20 30 40 50 60 70 80 Age World Health Organization (WHO) Osteoporosis Guidelines Bone Mineral Density Values Mean Lumbar Spine BMD: Decades 3 to 9 of a Woman’s Life T-Score WHO, Guidelines for Preclinical Evaluation and Clinical Trials in Osteoporosis, 1998. Adapted from AACE Guidelines. Endocr Pract. 2001;7:293-312.
DEXA scan: Hip T-Score
Who Should Be Tested? • All women aged 65 and older.* • Younger postmenopausal women with multiple risk factors • Postmenopausal women who present with fractures • Estrogen deficient women at clinical risk for osteoporosis • Individuals with vertebral abnormalities • Individuals receiving, or planning to receive, long-term glucocorticoid (steroid) therapy • Individuals with primary hyperparathyroidism • Individuals being monitored to assess the response or efficacy of an approved osteoporosis drug therapy. *Medicare covers BMD testing for the following individuals age 65 and older. Medicare permits individuals to repeat BMD testing every two years.
Risk Factors for Hip Fracture Skeletal Risk Factors for Fx Non-Skeletal Risk Factors for Falls/Fx -Age (>80 yr) -Poor balance/gait -Impaired eyesight -Meds that increase risk of falling -Loss of soft tissue hip padding -History of falls -Fall-related injury -Smoking Fx Risk -Low BMD (T< -2.5) -Previous Fx -Family history Fx -Smoking Risk of Hip Fx = Risk of Hip Fx =
Detection: Bone Mineral Density Tests Type of Test Area tested
Inhibitors of bone resorption: Calcium Estrogens +/- progest SERMs Bisphosphonates Calcitonin Stimulators of bone formation PTH Fluoride Therapeutic Agents Used in Osteoporosis • Normal Spine • B. Moderately Osteoporotic Spine • C. Severely Osteoporotic Spine
Bisphosphonates • Alendronate and alendronate plus vitamin D (brand name Fosamax® and Fosamax® plus D) • Ibandronate (brand name Boniva®) • Risedronate and risedronate with calcium (brand name Actonel® and Actonel® with Calcium) • Calcitonin (brand name Miacalcin®) • Mechanism of Action: • inhibition of the production of essential lipid compounds inside osteoclasts • decreased osteoclast activity • induction of cell death. • decreases bone turnover • slowing the rate at which new bone remodeling units are formed • reducing the depth of resorption. • increase in bone mass over time. Rodan, G. A. et al. J. Clin. Invest. 1996;97:2692-2696 Copyright ©1996 American Society for Clinical Investigation
Estrogen/Hormone Therapy Women's Health Initiative Trial • Hip and vertebral fractures decreased by at least one-third in both of the trials and total fractures decreased by 24%-30%. • The clear fracture benefits of postmenopausal hormone therapy (HT) are offset by the adverse effects: • increased risk of stroke, • cognitive impairment, and • deep vein thrombosis • HT provided no cardioprotective benefit, and increased the risk of breast cancer. (AMA) • Estrogens (brand names, such as Climara®, Estrace®, Estraderm®, Estratab®, Ogen®, Ortho-Est®, Premarin®, Vivelle® and others) • Estrogens and Progestins (brand names, such as Activella™, FemHrt®, Premphase®, Prempro® and others) • Parathyroid Hormone – Teriparatide (PTH (1-34) (brand name Fortéo®)
Combination therapy • The use of an anabolic and antiresorptive agent is less effective than an anabolic agent alone. • Since the effects of antiresorptive therapy with bisphosphonates are long-lasting, until more is known, bisphosphonate use should be discontinued before initiating PTH. • Combination therapy with two antiresorptive agents is generally reserved for those who: • have experienced a fracture while on therapy with a single drug • start out with a very low BMD and a history of multiple fractures • have a very low BMD and lose more bone mass on therapy with a single drug
Discuss calcium, vitamin D, nutrition, exercise. Discuss fall prevention Consider hip pads Already Fx? Rx Height loss >4cm? Xray Taking estrogen? No further work-up Hip DEXA or heel ultrasound Algorithm for women Older than 80 • Older women do not convert vitamin D in the skin & should be on an oral supplement • Check sedative use, vision, muscle weakness, balance, environmental problems (cords, rugs, poor lighting). Hip padding for thin women. yes • Raloxifene, calcitonin, or low-dose bisphosphonate. Do not start hormones. BMD not needed to decide treatment. no Fx yes No Fx no yes no
Counsel All Women on: • Risk factors for osteoporosis • Adequate calcium and vitamin D intake • The need for weight bearing exercise • Fall prevention strategies • Avoidance of tobacco and moderate use of alcohol • Consider Bone Mineral Density Screening for: • Women over 65 years of age • Women 50 to 64 with one or more of the following clinical risk factors • Any fracture after age 40 • Family history of osteoporosis • Current smoking • Weight <127 lbs. • Post-menopausal women who present with a fracture • Consider Treatment of Post-menopausal Women with: • T-score of < 2.5 or less • T-score of - 2.0 or less in the presence of one or more risk factors listed • Any vertebral or hip fractures • Web Resources • http://www.osteoed.org/ • Check out OsteoEd, an educational web site, for quick answers to osteoporosis questions. • *Guidelines from pamphlet for providers by the National Osteoporosis Foundation. http://www.nof.org/physguide/impact_and_overview.htm#synopsis Compiled by Judith ChilcotSchool of NursingUniversity of Washington Medical Center
Five Steps Toward Prevention 98% of a woman’s skeletal mass is acquired by age 20 Optimal strategies for building strong bones occurs during childhood and adolescence • A balanced diet rich in calcium and vitamin D • Weight-bearing and resistance-training exercises • A healthy lifestyle with no smoking or excessive alcohol intake • Talking to one’s healthcare professional about bone health • Bone density testing and medication when appropriate A study of disease management in a rural healthcare population demonstrated that a preventive program was able to reduce hip fractures and save money.
Prognosis • The best predictor of fracture is a previous fracture. • Treatment can improve fracture risk considerably. • Fractures can lead to decreased mobility and an additional risk of deep venous thrombosis and/or pulmonary embolism. • Vertebral fractures can lead to severe chronic pain of neurogenic origin, which can be hard to control. Although osteoporosis patients have an increased mortality rate due to the complications of fracture, most patients die with the disease rather than of it.


















