Download
1 / 18
230 likes | 856 Views
Medical Necessity and the Golden Thread . For Sweetser Affiliates Created by Nicole L. Dauphinee, LCPC (June 2015). Definitions of Medical Necessity. Federal Definition:

E N D
Medical Necessity and the Golden Thread For Sweetser Affiliates Created by Nicole L. Dauphinee, LCPC(June 2015)
Definitions of Medical Necessity Federal Definition: • any medical or remedial services (provided in a facility, a home, or other setting) recommended by a physician or other licensed practitioner of the healing arts, for the maximum reduction of physical or mental disability and restoration of an individual to the best possible functional level”(Federal Register, Section 1905(a)(13) of the Act and 42 CFR 440.130(d)).
Definitions of Medical Necessity continued… Maine’s definition: 1.provided in an appropriate setting; 2.recognized as standard medical care, based on national standards for best practices and safe, effective, quality care; 3.required for the diagnosis, prevention and/or treatment of illness, disability, infirmity or impairment and which are necessary to improve, restore or maintain health and well-being; 4. MaineCare covered service (subject to age, eligibility, and coverage restrictions as specified in other Sections of this manual as well as Prevention, Health Promotion and Optional Treatment requirements as detailed in Chapter II, Section 94 of this Manual); 5.performed by enrolled providers within their scope of licensure and/or certification; and 6.provided within the regulations of this Manual
Medical Necessity • “Simply stated, the documentation of medical necessity is the clear demonstration that there is a clinical need and that services provided are an appropriate response.” Treatment Planning for Person-Centered Care, Neal Adams, Diane M. Grieder, ElSevier Academic Press, 2005.
Utilization Review • An assessment of the medical necessity, efficiency and appropriateness of services and treatment plans on a prospective, concurrent, or retrospective basis.
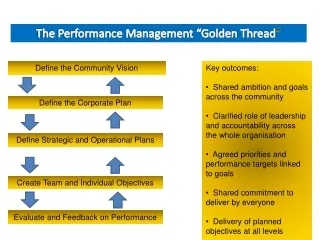
What are Sweeter’s Utilization Review Specialist and Manager seeking in chart audits? • “The Golden Thread” • All documents must be relevant to each other. • Assessed need (leads to) • Treatment recommendations (which leads to) • Treatment goals/objectives (which leads to) • Interventions (which leads to) • Progress
Creating an “invoice” • Our charts are our “invoices”. This is how we document the really good work that we are doing, in order to get properly compensated for that work. • For example, you wouldn’t pay a contractor for his work unless you saw an itemized bill explaining the services. Auditors/insurance companies don’t see our charts before we get paid; therefore, they can send an auditor to see the charts after the services have been paid for in order to determine if we have been properly paid for our services. If not, they will ask for money back for services not rendered. Even if the services were provided, but not documented, they did not happen in the eyes of an auditor.
Service Agreement • The Service Agreement includes information about services, payment policies, client’s rights, notice of privacy practices. • By going over the information with the client, you are essentially going over a contract for services to make sure that the client fully understands Sweetser policies, in addition to his/her rights in relation to accessing services.
Consents/Releases of Information • Signed permission to verbally discuss, disclose documentation, or obtain information from another person and/or agency. • Consents can be specific regarding what kind of information can be disclosed/obtained. • Document collaboration/conversations with others in progress notes, in order to show integrated care.
Adult and Adolescent AC-OK (and Substance Abuse Assessments) • AC-OK Screen for Co-Occurring Disorders assesses mental health, trauma, and substance abuse issues. The Adult AC-OK is for ages 21+; the Adolescent AC-OK (or OK-COD) is for ages 10-20. The AC-OK is a necessary document to be completed for all clients within the first 30 days of enrollment, preferably prior to the completion of the initial assessment. It is to be answered/completed by the client, in order to inform the assessment and treatment planning. The answers are in relation to the client’s experience in the last year. • If the client answers “yes” at least one time in the substance abuse section, then an additional substance abuse assessment may be warranted. If this turns out to be the case, then make sure to document in the Initial Assessment whether or not a referral for a substance abuse assessment was made, and the reasons why it was not (i.e. Client chose not to pursue a substance abuse assessment/counseling at this time; however, a referral shall be made at any time should the client change his/her mind.).
Initial Assessment • The Initial Assessment (IA) sets the stage for documenting the medically necessary work that you and the client will be accomplishing. • Due within the first 30 days of treatment. • 3 things need to be documented for medical necessity: • Presenting problem • Symptoms with a description (i.e. if the client is angry or anxious, then tell the reader what that looks like) • Functional status (i.e. how the symptoms are impacting the client’s functioning at home, school/work, and in the community).
Initial Assessment continued… • Clinical Summary and Formulation section: • Include the presenting problem, symptoms, and functioning. • Make sure to list enough symptoms so that you are proving/supporting the diagnoses given. • Clinical rationale for treatment (statement of medical necessity): • Note why outpatient mental health and/or substance abuse counseling is indicated and the expected benefit of the service to the client. • Make sure to note other services being recommended and/or already being accessed and/or why the client may be refusing such a recommendation.
Annuals and 90 day/Quarterly Reviews • Progress toward goals (i.e. possible goals that have been met that are being discontinued) • Barriers to meeting any goals • Any additions/changes to the treatment plan • Changes/new discoveries regarding symptoms/functioning which could affect the diagnoses being given • Interventions that have been helpful or not so helpful • Any explanations regarding gaps in treatment • Any recommendations for new services.
Diagnosis • Be specific with the diagnoses. If an NOS/Other Specified diagnosis is given, then it will need to be revised/adjusted with ongoing treatment. • Make sure to list enough symptoms in the Initial Assessment in order to prove/support the diagnoses given.
Mental Status • Make sure that the checkboxes match and line up with the diagnoses being given. • If suicidality/homicidality is indicated, then elaborate in the assessment: Current and history of plan, intent, attempts; risk and protective factors; detailed ICMP (Individual Crisis Management Plan) if appropriate.
Treatment Plan • The Treatment Plan connects back to the Assessment in the Golden Thread and operationalizes the agreed upon work that the client and clinician undertake to eliminate the symptoms and increase functioning. The Treatment Plan connects the client’s desired life’s change, (Long Term Goal (LTG)), with the more immediate work to be accomplished in the Short Term Goal (STG) as the client works towards discharge. Each goal is measurable and answers the question, “How will we know when we have reached this goal?” • Due within the first 30 days of treatment. • LTG- Client’s desired life change, for example, “I want to have more stable moods, be able to use coping skills to calm myself so I can talk to others when angry, and stop the self-talk that undermines my self-confidence and makes me depressed, so I can finish school and hold down a job.” (Could be several years out in order to fully accomplish). • STG- Measurable and attainable goal that the client agrees to accomplish in 3-6 months, in one to two review periods. For example, “Client will explore and name 3 triggers that begin a shift in mood.”
Treatment Plan continued… • Objective- The work that the clinician will perform, the intervention. For example, “Clinician will use CBT and DBT to support the client in managing moods.” • Discharge Criteria- The work that the client, clinician, and other team members agree upon accomplishing within a level of care time period, about 6- 12 months for OP Therapy. For example, “Client will discharge from therapy when he/she is able to use 3 coping skills regularly to control moods, attend school with less than 3 absences per quarter and maintain a part-time job for 3 months.” • The point of a Treatment Plan is to design a plan that incrementally guides the client and clinician to the LTG. The clinician and client may not be working together when the client meets their LTG because it may take several years to achieve the goal although the clinician will be a part of supporting them in their recovery journey and celebrating their successes along part of the way; hence, the STG’s that you will be working on slowly throughout the course of treatment and reviewing every 3 months/90 days.
Progress Notes • The Progress Note connects the dots in the Golden Thread back to the Treatment Plan and the work that the client and clinician agreed upon operationalizing in each session. • Each Progress Note records the following 4 necessary elements: • 1. The intervention: The action that you as the clinician are performing during the session and refers back to the Objective in the Treatment Plan. • 2. The response of the client to treatment (or the client’s response to the intervention) • 3. The progress towards the Short Term Goal: Rated each session (and can also be documented in the notes). • 4. The actual plan (and/or homework) for next session: A description of how you will be using your time together next session working towards meeting the Short Term Goal (homework for in between sessions can also be included)