Download
1 / 22
220 likes | 414 Views
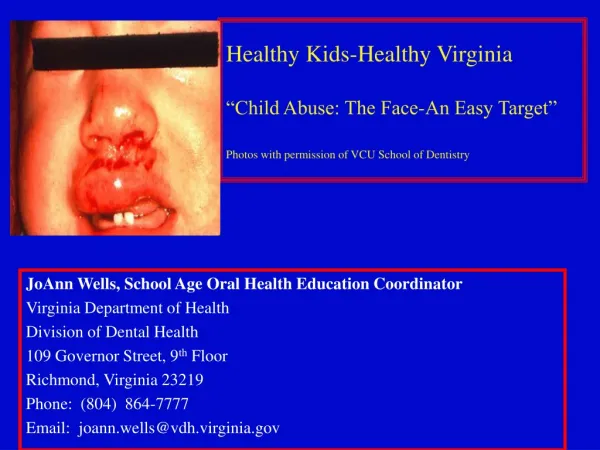
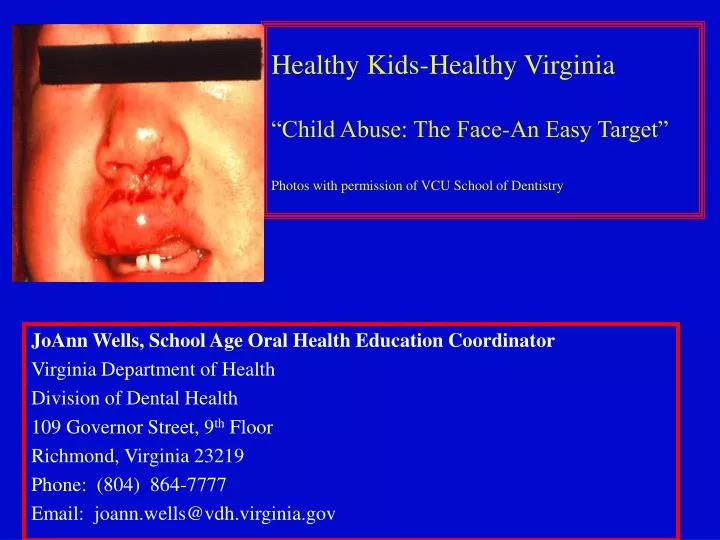
Healthy Kids-Healthy Virginia “Child Abuse: The Face-An Easy Target†Photos with permission of VCU School of Dentistry. JoAnn Wells, School Age Oral Health Education Coordinator Virginia Department of Health Division of Dental Health 109 Governor Street, 9 th Floor Richmond, Virginia 23219

E N D
Healthy Kids-Healthy Virginia“Child Abuse: The Face-An Easy Target”Photos with permission of VCU School of Dentistry JoAnn Wells, School Age Oral Health Education Coordinator Virginia Department of Health Division of Dental Health 109 Governor Street, 9th Floor Richmond, Virginia 23219 Phone: (804) 864-7777 Email: joann.wells@vdh.virginia.gov
The Problem: The Child’s View • 3 million children were reported abused or neglected in the US last year (Littel et al, 2004) • On the average, child abuse is reported every 10 seconds (Littel et al, 2004) • Child abuse and neglect is leading cause of death in children 4 and under (Littel et al, 2004) • 2,000 children died from abuse last year (Littel et al, 2004) • Maybe under-reported by one-half (Littel et al, 2004) 3 children die each day in a home in the US (Littel et al, 2004) Average age of the abused child is 3 years of age (Littel et al, 2004) Littel et al, 2004
The Problem: • Mandate to report • In all 50 states, dentists and dental hygienists are required to report suspected cases of child abuse and neglect (Kellogg et al., 2005) • Dental professionals have reported only 0.32% of all cases(Beem et al., 2005) -Only 1/2 of people report abuse when faced with an actual situation (Littel et al., 2004)
Until 19th century children considered property - no laws to protect children (Heins et al., 1984) 1871 - Mary Ellen, victim of abuse in New York City. No laws to protect children (Heins et al., 1984) A Church appealed to SPCA for help (Heins et al., 1984)
1962 - AAP sponsored symposium on child abuse Term “Battered Child Syndrome” proposed (Heins et al., 1984) 1974 - Child Abuse Prevention and Treatment Act passed (Heins et al., 1984)
Definition of Child Abuse • When a parent or other caregiver • Creates or inflicts, threatens or allows, a physical or mental injury by other than accidental means, or creates a substantial risk of death, disfigurement or impairment of bodily or mental functions • Commits or allows sexual exploitation of a child From VCA Sec. 63.1-248.2(A)
Consultation Dentist Child’s Physician Social Services (Kellogg et al., 2005)
RED FLAG Children with special needs are particularly vulnerable to abuse (Kenney et al., 2006)
Contributing Factors to Child Abuse • Drug and alcohol abuse • Stress • Lack of support network • Domestic violence • “Learned behaviors” - many abusers are, themselves, victims of child abuse (Kenney et al., 2006)
Possible Indicators of Child Abuse • Patterns • Bruises, welts, bite marks, tattoos • Lacerations or abrasions • Burns • Fractures • Head injuries (Kellogg el at., 2005) Photos with permission of VCU School of Dentistry
Warning Signs • Repeated injuries (multiple bruises) • Inappropriate behavior • Neglected appearance • Strict, super-critical parents • Extremely isolated families Kenney et al, 2006 Photos with permission of VCU School of Dentistry
Behavior Indicators of Abuse No eye contact Wary of parents Suicide attempts Dramatic mood changes INDICATORS Running away Fear of touch Aggressiveness Withdrawn (National Clearinghouse on Child Abuse and Neglect et al., 2003)
Clinical Protocol • General physical assessment • Behavior assessment • Patient history • Oral examination • Documentation • Consultation (Kenney et al., 2006)
Patient Histories • Obtain histories from child and parent. Do they match? • Is the injury consistent with the history? • History of similar injuries in the past? (Moudan & Smedstad et al., 2002)
24 hours 14 days Unintentional injury-child fell off bicycle (Kellogg et al., 2005) Photos with permission of VCU School of Dentistry
Physical Findings That Mimic Child Abuse • Genetic • Acquired • Accidental Facial hemangioma (Moudan & Smedstad et al., 2002) Photo by permission- VCU School of Dentsitry
Cultural Practices and Folk Medicine CAO GAO- hot coins rubbed over back or chest to cure fever (Morris et al., 2000) Photos permission of VCU School of Dentistry CUPPING- Warm cups are placed over the chest to draw out illness (Morris et al., 2000) Photos permission of VCU School of Dentistry
Signs of Oral Trauma in Abuse • Avulsed teeth • Non-vital teeth • Lip lacerations • Tongue injuries • Frenum injuries • Jaw fractures (Kellogg et al., 2005) Photos with permission of VCU School of Dentistry
Definition of Child Neglect • Neglecting or failing to provide care necessary for a child’s health • Abandonment (Kellogg et al., 2005) VCA Sec. 63.1-248.2(A) hotos with permission of VCU School of DentistryP
Identification of Dental Neglect • Willful failure of a parent or guardian to seek and follow with treatment necessary to ensure a level of oral health essential for adequate function and freedom from pain and infection • Untreated, rampant caries • Untreated pain, infection, bleeding or trauma • Lack of continuity of care once informed that above conditions exist (American Academy of Pediatric Dentistry Oral Health Policies and Guidelines, 2003) Photo by permission of VCU School of Dentistry
The Need For Education • 87% of dental professionals surveyed say they need more education about child maltreatment (Littel et al., 2004) • With education, dental professionals are five times more likely to report(Littel et al., 2004)
References American Academy of Pediatric Dentistry. Definition of dental neglect. Pediatric Dentistry. 2003; 25: 7. Beem, Marji H. (2005). The perceived likelihood of dental hygienist to report abuse before and after a training program. Journal of Dental Hygiene. 79. Dunn, A.M. (2002) Culture competence and the primary care provider. Journal of Pediatric Health Care. 16 (3), 105-111. Kellogg, Nancy. (2005). Oral & Dental aspects of child abuse & neglect. Pediatrics, 116 (6), 1565-1568. Kenney, John P. (2006). Domestic Violence: a complex health issue for dentistry today. Forensic Science International. 159, 121. Littel, Kristin. (2004). Family Violence: An intervention model for dental professionals. Office of Victims of Crime. Morris, Robert (2000) An unusual pattern of bruising (symmetric linear bruising caused by a folk medicine technique called coining). The Western Journal of Medicine. 172(5), 298. Moudan, L.D., & Smedstad, B. (2002) Reporting child abuse and neglect: the dental hygienist’s role. Dental Hygienist News. National Clearinghouse of Child Abuse and Neglect. (2005). Long-term consequences of child abuse and neglect. Virginia Department of Social Services. Professionals as mandated reporters & time frame for report & definition of Child abuse and neglect. Section 61.1-248.3 and 9-173.8.