Download

1 / 71
740 likes | 1.17k Views
Learn about HIV-associated infections, their diagnosis, treatment, and prophylaxis, focusing on Pneumocystis pneumonia.

E N D
Opportunistic Infections Associated with HIV Neelay Kothari, MD September 11th , 2017
HIV Epidemiology – United States • Estimated 1.1 million people living with HIV (2014) • 15% believed to be unaware of their infection • Males 75%, Females 25% • Rates of infection 8x higher amongst blacks than whites
Question AIDS causes defects primarily in which component of the immune system? • Granulocytes • Cell-mediated Immunity • Humoral Immunity • Macrophage activation • Mucosal protection
Question AIDS causes defects primarily in which component of the immune system? • Granulocytes • Cell-mediated Immunity • Humoral Immunity • Macrophage activation • Mucosal protection
OI approach in HIV • Reactivation of old infections • Herpesviruses / CMV • Tuberculosis • Increased risk of exposure • Hepatitis B and C • STDs • Increased risk of disease • Pneumocystis • JC virus
Case Presentation #1 • 34 year old Somali female with negative PMH • Two month history of progressive dyspnea, dry cough, headache, loss of appetite • Acutely worse over the past 3 days • Exam (pertinent positives) • Febrile to 102.9 degrees • Dyspneic and tachypneic • Scattered crackles on lung exam
Case Presentation #1 • There is a very extensive diffuse hazy ground-glass opacity in virtually all the lungs, more severely involving the dependent portion of the lower lung fields, atelectases, as well as mild air bronchogram
Case Presentation # 1 • Rapid HIV Test positive • CD4+ count = 14 • HIV Viral Load = 649,000
Case # 1: Differential Diagnosis • Which of the following is most likely? • (A) Pulmonary tuberculosis • (B) Pulmonary MAI infection • (C) Pneumocystis infection • (D) Toxoplasmosis pneumonia • (E) Cryptococcal pneumonia
Case 1: Diagnosis • How should diagnosis of pneumocystis pneumonia be made? • Blood fungal cultures • Sputum stain for pneumocystis • Sputum fungal cultures • Serology
Case Presentation #1 • Sputum stain positive for pneumocystis organisms
PNEUMOCYSTIS JIROVECI (CARINII) PNEUMONIA • CD4 < 200 in 90%; Mean CD4 = 79 • Before HAART: 70-80% got PCP without prophylaxis (mortality 20-40%) • Incidence markedly down with HAART • Risk of relapse 65 % w/o secondary prophylaxis
PNEUMOCYSTIS JIROVECI (CARINII) PNEUMONIA • Symptoms usually of insidious onset • Fever • Dyspnea • Non-productive cough • Often have oral thrush co-infection • Findings • Hypoxemia • Diffuse bilateral interstitial infiltrates (can have normal CXR) • LDH elevation (non-specific) • Pneumothorax
PNEUMOCYSTIS JIROVECI PNEUMONIA: Diagnosis • Histopathologic examination • PCR Testing • Beta-d-glucan assay • Not able to culture organism • Organisms persist for days to weeks • OK to start empiric treatment if high index of suspicion
Pneumocystis: Diagnosis • Histopathology (microscopy with staining): Sensitivity in HIV patients • Induced sputum 50-90% • Bronch with BAL 90-99% • Transbronch biopsy 95-100% • Open lung biopsy 95-100% • Lower yield in non-HIV patients • Lower organism burden
Pneumocystis: Diagnosis • PCR testing • Increased diagnostic yield, especially in non-HIV patients • Beta-d-glucan in serum • Up to 92% sensitivity • Not specific for pneumocystis
PCP Treatment • TMP-Sulfa is drug of choice • 15-20 mg/kg q6-8h x 21 days • Intolerance common (rash, pancytopenia, hepatitis) • Survival rate 91% if complete treatment • Other options (mild-to-moderate disease) • Dapsone + TMP (similar efficacy, more pills) • Primaquine + clindamycin • Pentamidine • Atovaquone • Other options (severe disease) • IV Pentamidine (more toxic – hypoglycemia, metabolic, hepatitis, pancreatitis, neutropenia) • Primaquine + clindamycin • Trimetrexate (not available anymore)
PCP TREATMENT • Allow 7-10 d for response; PATIENCE! • May deteriorate early • Keep dry! • Follow glucose on pentamidine • Steroids: If PO2 < 70 or A-a gradient > 35 mmHg • Reduced early deterioration in oxygenation, decreased early and intermediate mortality • Prednisone 40 mg bid x 5d,20 mg bid x 5 d, 20 mg qd to day 21
PCP PROPHYLAXIS • Indications for primary prophylaxis • CD4 < 200 (consider if 200-250 and dropping fast) • Oropharyngeal candidiasis • CD4 percentage < 14% • AIDS-defining illness without ART / viral suppression • Secondary prophylaxis • History of pneumocystis • Start immediately after completion of treatment regimen • Discontinuation • Once CD4 > 200 for at least 3 months • CD4 100-200 with consistent viral suppression for 3-6 months
Pneumocystis prophylaxis regimens • TMP-SMX 1 DS or SS daily • Dapsone 100 mg daily • Pentamidine Inhalation-300 mg q mo by neb • Non-compliant pts • More peripheral PCP and pneumothoraces • Atovaquone 1500 mg po daily • Dapsone + pyrimethamine + leucovorin • Atovaquone + pyrimethamine + leucovorin
Case 2: Same Patient • 2 years later…. • Patient presents with difficulty swallowing, mouth ulcers, weight loss, fever, and pain in chest • Has been non-adherent to HIV treatment and prophylactic medications, missed several clinic visits • CD4 count 20, HIV viral load > 100,000 • Exam: several ulcers in mouth, + thrush • Possible causes of patient’s symptoms?
Case 2: Continued • Admitted to hospital for evaluation • EGD • Multiple esophageal ulcerations • Perforation with possible tracheo-esophageal fistula • Biopsy -> CMV
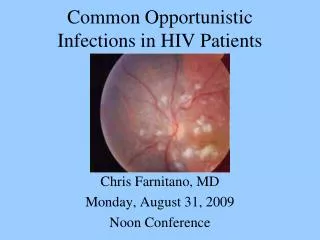
CMV • Typically causes disease with CD4 < 50 • Chorioretinitis • 30% incidence in AIDS patients (before HAART) • Initially unilateral – will spread to other eye • Floaters, visual loss, decreased acuity • Diagnosis: clinical ophthalmology evaluation • Treatment: systemic and local (val)ganciclovir • Esophagitis / colitis • Fever, weight loss, diarrhea, odynophagia • Can have hemorrhage / perforation rarely • Neurologic disease: dementia, ventriculoencephalitis, ascending polyradiculomyelopathy • Pulmonary disease: significance often unclear
Case Presentation #3 • 66 year old Native American male • Presenting with partial seizure with left face twitching, left arm rhythmic movements, and slurred speech • Past Medical History: CAD, hyperlipidemia, hypertension • Social History: divorced, works as mechanic and farmer, lives alone
Case Presentation #3 12 mm in diameter focus of ring enhancement at the corticomedullary junction of the lateral aspect of the precentral gyrus of the posterior right frontal lobe in the expected location of the primary motor cortex. There is vasogenic edema in the adjacent white matter of this gyrus
Case 3: • Differential Diagnosis? • Further workup?
Case Presentation #3 12 mm in diameter focus of ring enhancement at the corticomedullary junction of the lateral aspect of the precentral gyrus of the posterior right frontal lobe in the expected location of the primary motor cortex. There is vasogenic edema in the adjacent white matter of this gyrus 3 Days Later 1.1 cm peripherally enhancing lesion within the posterolateral right frontal lobe that has developed worsening non-enhancing increased T2 signal in the subcortical white matter compatible with edema
Case Presentation #3 • Laboratory Evaluation • HIV antibody POSITIVE • CD4 count = 32 • HIV viral load = 315,000 • Toxoplasma IgG POSITIVE
TOXOPLASMOSIS EPIDEMIOLOGY CLINICAL Disease risk CD 4 count usually < 50 33% will get disease without prophylaxis Symptoms Focal encephalitis Headache, confusion, focal motor weakness Fever Seizures ExtraCNS disease rare • Variable seroprevalence • 11% in United States • 50-75% in parts of Europe • Transmission • Undercooked meat with tissue cysts • Oocysts in cat feces (sporulation requires 24 hours) • Not person-to-person
TOXOPLASMOSIS-DIAGNOSIS • Clinical presentation • Serology 95 % sensitive • CT or MRI-Multiple, bilateral,hypodense, ring-enhancing mass lesions with predilection for B.G. and corticomedullary junction • Commonest cause of focal brain lesion in AIDS • Reduced in HAART Era • Clinical and radiographic response to Rx • Usually better in 2 wks
FOCAL BRAIN LESIONS IN HIV • Differential Diagnosis • CNS Lymphoma • Toxoplasmosis • Tuberculosis • Cryptococcus • Other: Bacterial / PML / Chagas disease • LP if safe and feasible • PCR: 96-100% sensitive, 50% specific • Often treat empirically for toxoplasmosis • Biopsy if fail to respond
TOXOPLASMOSIS:TREATMENT • Pyrimethamine(200mg x 1 then 50-100 mg qd) + Sulfadiazine(1-2 g q 6h) • Leucovorin to prevent BM suppression • 80-90 % respond in 2-6 wks • Relapse 90 % w/o maintenance • f/u CT or MRI in 2-4 wks • Treatment at least 6 weeks, often longer if incomplete response • Chronic maintenance / secondary prevention: Pyrimethamine 25-50 mg daily + sulfadiazine 2-4 grams daily + leucovorin • Other regimens • Pyrimethamine + Clindamycin • Pyrimethamine + Azithromycin or Clarithromycin • Atovaquone +/- Pyrimethamine
TOXOPLASMOSIS:PRIMARY PREVENTION • Indication: CD4 < 100 and Toxo IgG + • TMP-SMX 1 DS tab daily is first line • Other options • TMP-SMX 1 DS PO tiw • TMP-SMX 1 SS PO daily • Dapsone 50 mg PO daily + pyrimethamine 50 mg PO weekly + leucovorin 25 mg PO weekly • Dapsone 200 mg + pyrimethamine 75 mg + leucovorin 25 mg) PO weekly • Atovaquone 1,500 mg +/- pyrimethamine 25 mg + leucovorin 10 mg PO daily
Case Presentation #4 • 43 year old female originally from Kenya • 2-4 week history of • Left sided weakness • 10 lb weight loss • Mental slowing • Fatigue and sleepiness • Past medical history: anemia • Exam: slow to respond to questions, mild left sided weakness, white coating on tongue
Case Presentation #4 • Laboratory Evaluation • HIV Antibody POSITIVE • CD4 count = 16 • HIV Viral Load = 3,220,000 • RPR Negative • CSF • 1 WBC, 1 RBC, protein 26, glucose 54 • Cryptococcal antigen negative • JC virus PCR POSITIVE
Case # 4: Clinical Course • Patient was started on HIV treatment • Unfortunately her mental status continued to deteriorate • Transitioned to comfort care and died
PROGRESSIVE MULTIFOCAL LEUKOENCEPHALOPATHY • JC Virus – 85% of population seropositive • CD4+ count usually < 100 • Clinical Presentation • Demyelinating lesions • Focal neurologic deficits • Progressive over weeks to months • Seizures in 20% • Imaging: • Multiple nonenhancing white matter lesions • No mass effect • CSF analysis: PCR positive in 70-90% if not on HAART
PROGRESSIVE MULTIFOCAL LEUKOENCEPHALOPATHY • Treatment • No specific treatment • Reverse immunosuppression • Start HAART immediately • Prognosis • High morbidity and mortality • Half get better with HAART, though often have residual deficits • Lower CD4 count at presentation associated with poor outcome
Immune Reconstitution Inflammatory Syndrome (IRIS) • Parodoxical clinical worsening after starting HAART despite improved immune function • Due to inflammatory response against infectious antigen • CD 4 count usually < 50 • Usually within 6 weeks, though can be several months • Common pathogens: MAC, TB, CMV, cryptococcus, pneumocystis, JC virus • Can have atypical presentation • Treatment: continue HAART if possible, treat infection, anti-inflammatory therapy
Case Presentation #5 • 46 year old male previously healthy • Chief complaint: headache • Present for approximately one month • Sudden onset, with gradual worsening since • Bilateral, retro-orbital and into top of head • Initially seen in Minute Clinic • Presumed sinusitis, prescribed amoxicillin • Not better, prescribed azithromycin • Not better, then prescribed Vicodin 6 days prior to admission
Case Presentation #5 • Associated symptoms • Nausea and vomiting x 2 weeks • 15 pound weight loss • Brief 30-60 second episodes of dizziness • Intermittent photophobia • Ringing sensation in right ear • Feels somewhat depressed • Per family • Slow mentation and speech • Increased sleepiness
Case Presentation #5 • Works as nail technician, unable to work recently • No tobacco, occasional cigar, occasional alcohol (2 drinks per week), denies other drug use • Travel: recent travel to England • No pets, animal or tick exposures, sick contacts • Enjoys gardening
Case Presentation #5 • VS Temp 98.1, P 75, R 16, BP 131/90 • Weight 130 lb • General: flat and depressed affect, slow speech • HEENT: whitish patches on tongue • Skin: 3-4 mm skin colored papules present on forehead, shoulder, sternum • Remainder of exam unremarkable
Case Presentation #5 • HEAD MRI • Focally increased signal intensity on FLAIR and T2-weighted images involving the caudate nuclei, putamina, globuspallidus nuclei and the thalami bilaterally. • No associated hemorrhage, midline shift or hydrocephalus. • Patchy restricted diffusion in the same distribution, but to a lesser extent than the areas of T2 prolongation.
Case Presentation #5 • HEAD MRI • Focally increased signal intensity on FLAIR and T2-weighted images involving the caudate nuclei, putamina, globuspallidus nuclei and the thalami bilaterally. • No associated hemorrhage, midline shift or hydrocephalus. • Patchy restricted diffusion in the same distribution, but to a lesser extent than the areas of T2 prolongation.