Download
1 / 52
600 likes | 1.47k Views
INTRODUCTION TO CONTINUOUS GLUCOSE MONITORS. H. Peter Chase, MD Vicky Gage, RN, CDE Laurel Messer, RN, CDE Susie Owen, RN, CDE Sally Sullivan, RN, CDE. Barbara Davis Center for Childhood Diabetes April 2010. Agenda. Dr. Chase will present a general CGM overview

E N D
INTRODUCTION TO CONTINUOUS GLUCOSE MONITORS H. Peter Chase, MD Vicky Gage, RN, CDE Laurel Messer, RN, CDE Susie Owen, RN, CDE Sally Sullivan, RN, CDE Barbara Davis Center for Childhood Diabetes April 2010
Agenda • Dr. Chase will present a general CGM overview • Nurses will explain device features and comparisons between sensors • You will have an opportunity to handle each device and ask questions Barbara Davis Center for Childhood Diabetes April 2010
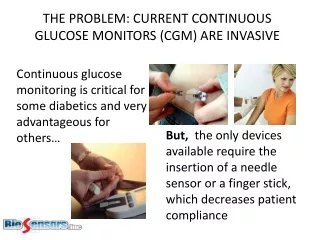
What is a CGM? (Continuous Glucose Monitor) • A device that provides “real-time” glucose readings and data about trends in glucose levels • Reads the glucose levels under the skin every 1-5 minutes (10-15 minute delay) • Provides alarms for high and low glucose levels and trend information • The 3rd era in diabetes management Barbara Davis Center for Childhood Diabetes April 2010
Who Should Use a CGM? • The person and the family must both want a CGM • A youth must be willing to wear the sensor (and carry the receiver) • Using good diabetes care (4 BGs/day) • Good support system • Adequate body “real estate” • Cost of CGM (RNs to elaborate) Understanding Pumps and CGMs, p.100 Barbara Davis Center for Childhood Diabetes April 2010
WHY Use CGM? • Prevention of low blood sugars (alarms) • Prevention of high blood sugars (ketones) • Minimize wide glucose fluctuations • Behavior Modification • Prevention of Complications (?) Barbara Davis Center for Childhood Diabetes April 2010
How common are glucose levels <60mg/dl during the night in children with T1D? • French (i) and Australian (ii) data showed approximately 50% of children with low BG (<60mg/dl) during the night (on NPH bid) • DirecNet data (one night in hospital with blood sugars every 30 min.) A) 2001-2002: 39 of 91 (43%) low BG (44% of children on insulin pumps/56% on NPH) B) 2004: 14 of 50 (28%) with low BG (all on insulin pumps or Lantus) (i) Beregszaszi M, et al. J Pediatr. 131, 27, 1997 (ii) Porter PA, et al. J. Pediatr. 13, 366, 1997 Barbara Davis Center for Childhood Diabetes April 2010
WHY Use CGM? • Prevention of low blood sugars (alarms) • Prevention of high blood sugars (ketones) • Minimize wide glucose fluctuations • Behavior Modification • Prevention of Complications (?) Barbara Davis Center for Childhood Diabetes April 2010
“Snapshot of BG levels” Barbara Davis Center for Childhood Diabetes April 2010
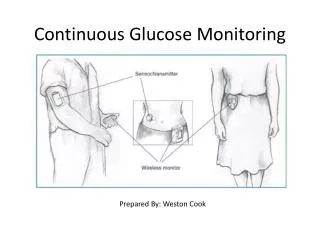
Continuous Glucose Monitoring Barbara Davis Center for Childhood Diabetes April 2010
< 180 181 - 240 241 - 300 > 300 Hyperglycemia is common, especially after meals 50% 40% 30% Breakfast Lunch 20% Dinner 10% 0% Boland et al, Diabetes Care 24:1858, 2001 Barbara Davis Center for Childhood Diabetes April 2010
WHY Use CGM? • Prevention of low blood sugars (alarms) • Prevention of high blood sugars (ketones) • Minimize wide glucose fluctuations • Behavior Modification • Prevention of Complications? Barbara Davis Center for Childhood Diabetes April 2010
Three Parts to CGMs: • Sensor • Transmitter • Receiver/Monitor Understanding Pumps and CGMs, p.103 Barbara Davis Center for Childhood Diabetes April 2010
Sensor • (p.103) Barbara Davis Center for Childhood Diabetes April 2010
B) Transmitter (p.103) Barbara Davis Center for Childhood Diabetes April 2010
C) Receiver or Monitor (p.103) Barbara Davis Center for Childhood Diabetes April 2010
What does “Calibration” mean and why do I need to do it? • Calibration is a process that gives a fingerstick BG value to the CGM system so the values will align with each other • Number of Calibrations vary by device • Best times to calibrate are when the BG values are stable: before meals and before bed • Do not calibrate when arrows are present Barbara Davis Center for Childhood Diabetes April 2010
What type of data will we get? • Two types of CGM data: • Real Time data: seen on CGM • Retrospective data: download to a computer Barbara Davis Center for Childhood Diabetes April 2010
Real Time Data Three types of Real Time Data: A) Trend graphs B) Alarms C) Trend Arrows Understanding Pumps and CGM: pages 109-113 Barbara Davis Center for Childhood Diabetes April 2010
Real Time data TREND GRAPHS Trend graphs – Knowing a glucose level is 240 mg/dl may not be as important as knowing the “trend.” Understanding Pumps and CGM: p.103 Barbara Davis Center for Childhood Diabetes April 2010
ALARMS Real Time data Warn patients of current or projected high and low blood sugar Barbara Davis Center for Childhood Diabetes April 2010
Real Time data Alarms continued Threshold alarm: Warning when glucose is above or below a set value --all devices have this Projected Alarms: 10,20 or 30 minute warning of Impending hypo- or hyperglycemia Real-Time Revel System, Guardian Real-Time and the Navigator have these Barbara Davis Center for Childhood Diabetes April 2010
Real Time data TREND ARROWS Arrows that indicate the rate and direction of change Glucose rising quickly >2 (mg/dL)/min Glucose going up 1 to 2 (mg/dL)/min Fairly stable glucose -1 to 1 (mg/dL)/min Glucose going down -1 to -2 (mg/dL)/min Glucose falling quickly >-2 (mg/dL)/min Barbara Davis Center for Childhood Diabetes April 2010
Retrospective Data Three types of Retrospective data (viewed on computer download) • Trend graphs • Pie charts • Data tables Understanding Pumps and CGMs, Chapter 17 Barbara Davis Center for Childhood Diabetes April 2010
Retrospective data A) Trend Graphs Reports that show one or more days of CGM data– also called sensor overlay Barbara Davis Center for Childhood Diabetes August 2009 Barbara Davis Center for Childhood Diabetes April 2010
Retrospective data Case Study:Using Trend Graphs • Three Trend Graphs showing change over time: • Teenager with T1D for 9.5 years • Started Navigator: Sept. 2005 • Starting HbA1c: 7.1% • Most recent HbA1c: 6.0% • Current number of low BGs per week (<60 mg/dL or <3.3 mmol/L): 1/week Barbara Davis Center for Childhood Diabetes April 2010
Retrospective data BASELINE GLUCOSE Trend Graph #1Prior to CGM Use Barbara Davis Center for Childhood Diabetes April 2010
Glucose Trend Graph #2After three months of CGM use Retrospective data Barbara Davis Center for Childhood Diabetes April 2010
GLUCOSE Trend Graph #3Most recent CGM report Retrospective data Barbara Davis Center for Childhood Diabetes April 2010
Retrospectivedata B) PIE CHARTS Show percentage of time glucose is above, below and in target range Barbara Davis Center for Childhood Diabetes April 2010
Retrospective data C) Data Tables Show statistical information about different periods of the day Barbara Davis Center for Childhood Diabetes April 2010
USING CGM RESULTS: (To make insulin adjustments) • Important not to get overwhelmed by data • ** Make One Change At A Time • Look for patterns 2 out of 3 days • A behavior modification device Missed boluses, snacking, low BGs on CGM • Good initial communication with HCP Barbara Davis Center for Childhood Diabetes April 2010
Interpreting CGM data Barbara Davis Center for Childhood Diabetes April 2010
Interpreting CGM data Barbara Davis Center for Childhood Diabetes April 2010
Realistic Expectations of CGM • You will still need to test your blood sugar levels • Using CGM does not make Diabetes Management a “Breeze” • You will still experience low and high blood sugar values • Sensor values will not always “MATCH” the blood sugar values • The most significant improvements will be seen with consistent CGM wear Barbara Davis Center for Childhood Diabetes April 2010
Realistic Expectations of CGM You will still need to test your blood sugar levels for: • Calibrations • Insulin dosing • Treating high and low blood sugar levels • Questioning the accuracy of the CGM values • Times when you do not feel right Barbara Davis Center for Childhood Diabetes April 2010
Realistic Expectations of CGM Using CGM does not make Diabetes Management a “Breeze” • Initially, people are overwhelmed from all the data • Subjects will follow an algorithm early on in the use of CGM • Family weekly downloads of CGM data are important • CGM works as a behavior modification device Barbara Davis Center for Childhood Diabetes April 2010
Realistic Expectations of CGM You will still experience low and high blood sugar levels • There will ALWAYS be some lows and highs • Alarms may NOT be sensitive to slowly falling blood sugar values • The time spent in hypoglycemia and hyperglycemia can be reduced • CGM is an additional tool to help make decisions • CGM values are not very helpful in treating lows Barbara Davis Center for Childhood Diabetes April 2010
Realistic Expectations of CGM • Sensor values will not always “MATCH” the blood sugar values • CGM values are about 10 minutes behind blood sugar values • Values are less accurate early after insertion • Values are furthest off when blood sugars are rapidly rising or falling • Calibrations are important determinants of accuracy of the CGM Barbara Davis Center for Childhood Diabetes April 2010
Realistic Expectations of CGM The most significant improvements will be seen with consistent CGM wear ( >6 days/week) • Good initial education helps patients and families to learn what to expect • Regular use of Real-time and Retrospective data is necessary for optimal benefits • Follow up with Diabetes Team is important to continue to make adjustments Barbara Davis Center for Childhood Diabetes April 2010
Questions? • Next: Device Information from the nurses • Hands on with CGM devices Barbara Davis Center for Childhood Diabetes April 2010
CGMs availableApril 2010 Barbara Davis Center for Childhood Diabetes April 2010
Paradigm Real Time systems(Paradigm pump and Revel pump) • A: Insulin pump and CGM receiver • B: Infusion set • C: Sensor • D: Transmitter Barbara Davis Center for Childhood Diabetes April 2010
Paradigm Real-Time system(Paradigm pump and Revel pump) • Pump is not controlled by CGM readings • No extra receiver to carry • Has high and low alarms • Revel has predictive alarms • Sensors last 3 days (6 days) • Calibrations every 12 hours • Great online download Barbara Davis Center for Childhood Diabetes April 2010
Guardian Real Time • For people not using a pump • Has high and low alarms • Has predictive alarms • Sensor lasts 3 days (6 days) • Calibrations every 12 hours • Why not buy a pump? Barbara Davis Center for Childhood Diabetes April 2010
Navigator CGM Barbara Davis Center for Childhood Diabetes April 2010
Navigator CGM • Has built in Freestyle BG meter • Larger transmitter • Has high and low alarms • Has predictive alarms • Sensors last 5 days • Calibrations at 10, 12, 24 and 72 hours • Well studied and highly accurate Barbara Davis Center for Childhood Diabetes April 2010
DexCom 7 Plus Barbara Davis Center for Childhood Diabetes April 2010
DexCom 7 Plus • Most simple system to use • Smallest transmitter • Has high and low alarms • Has rate of change alarms • Sensor lasts 7 days • Calibrations every 12 hours • Basic download software Barbara Davis Center for Childhood Diabetes April 2010
CGM Reimbursement Family will fill out an Authorization to release insurance information Physician will write prescription (Letter of Medical Necessity) BDC will provide any other paperwork requested by the insurance company Call Mireya at BDC to get started phone: 303-724-6763, fax: 303-724-6779 Barbara Davis Center for Childhood Diabetes April 2010