Download
1 / 15
150 likes | 676 Views
Optimizing the Periosteal Flap for Lateral Eyelid Reconstruction. W. Thomas McClellan, M.D., WVU Clinton McCord, M.D., Emory Rebecca Neusch, WVU Nothing to Disclose. Objective of the Study.

E N D
Optimizing the Periosteal Flap for Lateral Eyelid Reconstruction W. Thomas McClellan, M.D., WVU Clinton McCord, M.D., Emory Rebecca Neusch, WVU Nothing to Disclose
Objective of the Study To establish a standardized method to harvest the periosteal flap in order to improve eyelid strength, position, and reduce ectropion.
Materials and Methods - Design • Create a central meridian from the upper puncta to the lateral orbital rim. • This intersection point is where the superior aspect of the flap is started and continues at a 40 degree angle superiorly out a distance X (which is the length needed to repair the defect).
Materials and Methods - Design • The width of the flap should measure 6-7 mm which compensates for primary contracture while maintaining strength of the periosteum. The periosteum is then secured with 5-0 Vicryl to the lateral edge of the tarsal plate with enough tension that the lid approximates the globe.
Materials and Methods - Design • If the flap is extended onto the temporalis fascia up to 50% of the posterior lamella of the lower eyelid can potentially be closed.
Materials and Methods • Once the flap is secured, a Tenzel flap can be rotated to repair the anterior lamellar defect and sutured with 6-0 nylon and 5-0 plain gut near the line margin. • Sutures are removed at 6 days.
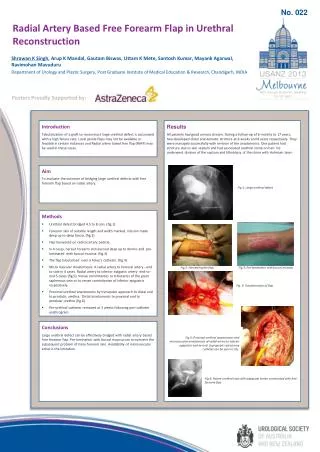
Surgical Images Figure 1 Pre-Op 80% lower eyelid + canthal Defect Figure 2 Intra-Op periosteal flap dissection
Surgical Images Figure 3 Periosteal flap reflected to bridge the posterior lamellar defect
Post-Operative Images Figure 4 Post-Operative Frontal View Figure 5 Post-Operative Oblique View
Results and Conclusions • 12 patients all with good outcomes • There were no complications such as canthal dehiscence, cicatrical ectropion or entropion.
Results and Conclusion • The periosteal flap is an ideal flap to repair the lateral canthus and lateral posterior lamella due to its simplicity, reliability, and low risk.
Results and Conclusion • It can be designed to match the native eyelid contour, originates within the lateral orbit, is strong, and highly vascular2. Additionally if the flap relaxes with time it can be elevated and re-secured within the lateral orbit.
Significance of the Findings This standardized method demonstrates a reliable method of reconstructing lateral eyelid defects. It optimizes lid position and reduces post operative ectropion.
References 1. Smith, B.C., Nesi, F.A. Practical Techniques in Ophthalmic Plastic Surgery. St. Louis: The C.V. Mosby Company, 1981. Pp. 92-95. 2. Weinstein GS, Anderson RL, Tse DT, Kersten RC. The use of a periosteal strip for eyelid reconstruction. Arch. Ophthalmol. 1985 Mar;103(3):357-359. 3. McCord, C.D. Jr., Codner, M.A. Eyelid and Periorbital Surgery, Vol.2, 1st Ed. St. Louis: Quality Medical Publishing, Inc., 2008. Pp. 600.