Download
1 / 12
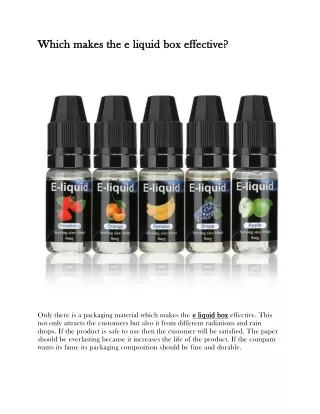
120 likes | 238 Views
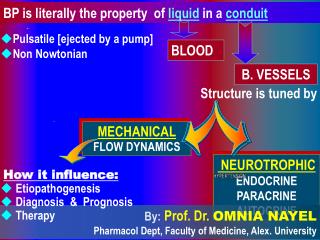
MECHANICAL FLOW DYNAMICS. NEUROTROPHIC ENDOCRINE PARACRINE AUTOCRINE. BP is literally the property of liquid in a conduit. Pulsatile [ejected by a pump] Non Nowtonian. BLOOD. B. VESSELS. Structure is tuned by. How it influence: Etiopathogenesis Diagnosis & Prognosis Therapy.

E N D
MECHANICAL FLOW DYNAMICS NEUROTROPHIC ENDOCRINE PARACRINE AUTOCRINE BP is literally the property of liquid in a conduit • Pulsatile [ejected by a pump] • Non Nowtonian BLOOD B. VESSELS Structure is tuned by How it influence: • Etiopathogenesis • Diagnosis & Prognosis • Therapy By:Prof. Dr. OMNIA NAYEL Pharmacol Dept, Faculty of Medicine, Alex. University
Normally FLOW DYNAMICS comprises Shear Stress Tensile Stress =Cyclic Stretch SS: is a friction force acting on the interface between flowing blood & vessel wall, due to the drag between the thin stationary layer of fluid adjacent to the luminal endothelial surface and the outer layers of moving blood. CS: is a tensile strain [stretch] imposed circumferentially at right angles to blood flowing in vessel. It propagates along the longitudinal axes of the vessel. It is cyclic due to the rhythmic distension and expansion of arteries / cardiac cycle It is governed by the varied arterial properties: • Dispensability • Compliance Dispensability: Fraction change in arterial caliber as pressure change; it is a determinant of pulsatile stress on the vessel wall & reflects the yielding property of the artery. Compliance: The magnitude increase in artery dimension in response to an increment in pressure & reflects the buffering capacity of the artery.
CAPACITANT VESSELS: are normally compliant structures capable of buffering BP changes that occur during the cardiac cycle [SBP/DBP (PP) ] to maintain distribution of tissue BF via the CONDUIT VESSELS. Capillaries Arterioles RESISTANCE VESSELS < 400 mm > 400 mm The rate at which the created AORTIC PRESSURE WAVES travel PULSE WAVE VELOCITY(PWV) SS generated by each PW excites the release of a spurt of NO allowing balanced tone that ensures: *Forward progression of PW more distally to pertain the peripheral tissue distribution. * Limit / delay the amplitude of RW to reach during diastole to pertain CBF. This pulse wave is then REFLECTED from periphery as a REFLECTION WAVE (RW) and normally returns in diastole, thus serving to maintain CBF.
VASOCONSTRICTION • BLUNTED NO - MEDIATED VASODILATATION Fracture & fragmentation of elastic lamillae Hypertrophic & Euotrophic Remodeling Endothelial Dysfunction Disturbed Flow Dynamics IN HYPERTENSION ACUTE VASOMOTOR TONE CHANGES CHRONIC VESSEL RESTRUCTURING I I I I I I I I Vessels are capable of: • SENSING by mechanosensorsIntegrin • TRANSDUCING it Mechanically/Chemically • TRANSLATING it to a Response whether - acute Functional - chronic Structural ?
IA: How different mechanosensor integrins perpetuate the etiopathogenisis of hypertension ? . . . . . SS . . . . . . . . . . CS Rapid mechanotransduction Integrin a1 b1, a5 b1 . . . . Integrin avb3 Mechanical constrain [SS & CS ] are important determinants in Vasomotor Alteration & Vessel Remodeling J Vasc Res 2000 Aug: 37: 147-57. Hypertension 2000 Sept; 36: 312-18. Circulation 2001 Jan ; 103: 597-603. Delayed Adaptive Responses [ 20 min. - 1hrs] . . . . . Am J Physiol Endocrinol Metab 2002; 282: E1-E10
IB:How does such structure alteration perpetuate more etiopathogenic flow disturbance in hypertension. Fracture & fragmentation of elastic lamillae PWV Widening PP Stiffen Hypertrophic & Euotrophic Remodeling Amplitude of RW This accelerates it to arrive at systole This leads to its summation with the Aortic Pulse Wave Central Peak Systolic Pressure > Brachial BP Ventricular Hypertrophy
IIA:How does measurement of flow dynamics[CS] aid in diagnosis & prognosis of hypertension ARTERIAL STIFFNESS vs COMPLIANCE Best indexed by PULSE WAVE ANALYSIS [PWA]of ARTERIAL PRESSURE WAVEFORM using a recently-developed computerized, portable simple-to-use device [SphygmoCor ]. Recording of radial, carotid, femoral … waveform is achieved by an applanation tonometry; composed of a hand-held pencil type probe incorporating a high fidelity strain-gauge transducer at the tip of which is a small pressure sensitive ceramic sensor area. It is applied by gentle pressure at max pulsating area against underlying bone / 10 consecutive beats to cover a resp. cyc. From the P wavefrom recordings the Augmentation Index[AIx] is calculated = Difference between 1st & 2nd systolic pressure [SP] expressed as % of PP. It is attributable to RW.
Augmentation Index [AIx] -ve in young / zero at 35y / +ve thereafter Reveals extent of ED Measures addition load imposed on LV due to RW / correlated with LVM Partly depend on PWV which is # to dispensability / compliance Partly dependent on EF & duration Partly dependent on amount & site ofRW (m. art. / arterioles) > Higher in women ??? Because they are of shorter stature Short stature [>RW] is a risk to CVD !!!!!!
IIA:How does measurement of flow dynamics[CS] aid in diagnosis & prognosis of hypertension Complior Device (Colson) Also indexed by PWV determination ARTERIAL STIFFNESS vs COMPLIANCE Using a foot-to-foot flow wave velocity method through application of TWO TRANSDUCERS with known distant apart HR – related variation of PWV may be limiting for its use in clinical trials assessing arterial stiffness !!! It is +ve correlated with BP & Age That is why in JNC 7 report [Age (>55 y/ men, >65 y / women) is one of the major CV risk factors because PP & PWV(JAMA. 2003;289) Molecular biology recently cleared that men with shorter telomere length are prone to PP & PWV artery stiffness
IIB:How does measurement of flow dynamics[SS] aid in diagnosis & prognosis of hypertension Positions of the sample volume Equals the distance between the leading edge of the echo produced by the intima-lumen interface of the near wall and that produced by the lumen-intima interface of the far wall. By:Cone / Plate Viscometer By: High Resolution Echo Doppler Applied at common carotid arteries 1 to 2 cm proximal to the bulb. BFV recorded in different sites across the arterial lumen BF profile drawn according to velocity values SS = Blood viscosity x Blood velocity / Internal diameter SS is directly proportional to • Blood viscosity [Rheology] • Velocity gradient of the arterial wall Inversely proportional to • Vessel diameter Internal diameter is measured just before and during the systolic wave passage of cardiac cycle i.e at the narrowest vs largest luminal diameter and the mean is taken. N.B.SS can arbitrary be indexed using Forearm BF by Plethmography
III:How does knowledge on flow dynamics aid in choice & innovations of antihypertensve therapy MODIFYING MECHANOTRANSDUCTION NITRATES INTEGRINS Improve COMPLIANCE by affecting AIx RW through its role on conduit arteries & arterioles. ANTI - INTEGRINS Monoclonal Ab or Peptide Inhibitors against them. Recombinant Bioengineering. Normalization of vessel function & structure is a deemed goal so interplaying on the flow dynamics should be considered. It was for long thought that COMPLIANCE is better achieved by the use of CCBs, vasodilators, ACIs/ARBs >selective b-blockers and just some diuretics !!!!! But now it is proved that
III:How does knowledge on flow dynamics aid in adopting a preventive therapy tohypertension SS C S T H A N K EXERCISE is an ANTIDOTE for HYPERTENSION • NO • IS & GLUT • Sk. m. capillarity • TG LDL HDL oxid. enz • Cytokines & Inflammation • ROS Y O U