Download
1 / 16
160 likes | 184 Views
Explore the key concepts of adaptive immunity, including B cells, antibodies, age-related changes, neutralization of toxins, viruses, and bacteria, Fc receptors, and two intriguing medical case studies.

E N D
ADAPTIVE IMMUNITY: B CELLS AND ANTIBODIES March 31, 2009 10:00-11:00
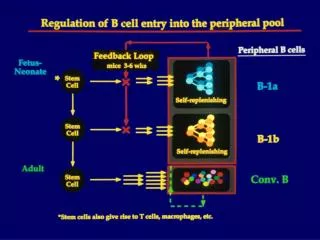
AGE ASSOCIATED CHANGES IN SERUM Ig LEVEL In utero and at birth maternal Ig protects infants Infants do not make Ig until approximately 6 months
ANATOMICAL LOCATIONS OF ISOTYPES OF Ig Fc portions of Ig determine anatomical location and function of isotypes IgG and IgM predominate in plasma IgE is associated with epithelial surfaces IgA predominates in mucosal secretions
THE POLY-Ig RECEPTOR MEDIATES TRANSCYTOSIS Transcytosis is the unidirectional transport of macromolecules through a cell IgM can also be transported across epithelial cells
THE BRAMBEL RECEPTOR TRANSPORTS IgG INTO EXTRACELLULAR SPACES
NEUTRALIZATION OF TOXINS IgM, IgG and IgA can neutralize toxins Many pathogens produce toxins Immunization with toxoid (inactivated toxin) protects against tetanus and diptheria
NEUTRALIZATION OF VIRUSES IgM, IgG, and IgA can neutralize viruses
NEUTRALIZATION OF BACTERIA IgM, IgG and IgA can neutralize bacteria
CHARACTERISTICS OF FcR Two broad types: Inhibitory and Activating Inhibitory FcR have ITIMs on cytoplasmic domains Activating signal through a “common” g chain containing an ITAM Most FcR interact the stongest with IgG1 Exceptions: Fce and Fca FcR have restricted expression Most types of FcR are on macrophages and neutrophils Mast cells only have Fce
FcR ON PHAGOCYTES FACILITATE ELIMINATION OF PATHOGENS Phagocytes have receptors for IgG FcR interact with IgG coated pathogens and increase the efficiency of phagocytosis: OPSONIZATION
IgE BINDS FceR ON MAST CELLS Crosslinking FceR results in release of inflammatory mediators
ADCC IgG1 binds to target cells Interaction with FcR on NK cell juxtaposes the target and NK NK gets turned on and kills the target
Bill Grignard: An M1 Without Antibodies Bill was healthy for the first 10 months of his life. At that time he started to have infections which were treated successfully with antibiotics. He was bright, active and continued to grow despite repeated ear infections and 2 bouts of pneumonia. At age 2 he was tested for serum Igs: 80mg/dl IgG normal (600-1500); no IgA, and 10 mg/dl IgM (normal 75-150). He was treated with i.m. injections of gamma globulin. At age 9 he was referred to you for a chronic cough. You observed an absence of tonsils (not removed). His WBC was normal. A family history revealed that he had a brother with a similar problem, and two uncles who died of infections when they were young. Bill was diagnosed with XLA (Btk deficiency). He injects himself daily with gamma globulins. • Why was Bill healthy until 10 months? • Why doesn’t he have tonsils (he did not have a tonsillectomy)? • If you isolated lymphocyte precursors from his bone marrow and • looked at the Ig gene loci, would you find evidence of Ig gene • rearrangement? • What other genetic defects could lead to arrested B cell development • at the same stage as Btk deficiency?
Dennis Fawcett: A Boy Who Can’t Switch Dennis was referred to you when he was 5, but he had suffered recurrent infections since he was 1. He was admitted to the hospital with a severe acute sinus infection. Interestingly, despite the infections his WBC was normal. Interestingly, antibodies to the infectious agent (Streptococcus) were not present in his serum 7 days later. Total serum Ig levels were: IgM-210 (normal 75- 150) IgA-0; IgG 25 (normal 600-1500). Lymph node biopsies revealed poorly organized structures and no GC. Dennis received a booster shot for diptheria, tetanus, and pertussis toxoids. 14 days later, no anti-toxoid was detected. He did have serum antibodies to appropriate blood groups (carbohydrates). FACS showed he had B cells and T cells. His T cells did not bind CD4O. • Dennis’ B cells expressed IgM and IgD. Why didn’t have difficulty switching • from IgM to IgD? • Why did Dennis make antibodies to blood group antigens, but not toxoids? • Why is IgG more effective at fighting this type of bacterial infection than IgM? • During an infection, would you expect Dennis to have enlarged lymph nodes?