Download
1 / 16
160 likes | 165 Views
This study examines the scope and severity of serious infections (SIE) in patients with immune-mediated inflammatory diseases (IMID) receiving TNF inhibitors (TNFi). The results show a small increased risk of opportunistic and bone/joint infections in TNFi-treated patients, with greater SIE severity and longer hospitalizations.

E N D
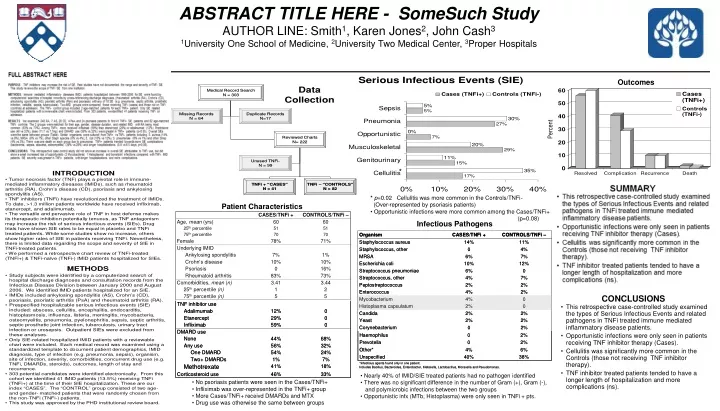
ABSTRACT TITLE HERE - SomeSuch Study AUTHOR LINE: Smith1, Karen Jones2, John Cash3 1University One School of Medicine, 2University Two Medical Center, 3Proper Hospitals * * p=0.02 Cellulitis was more common in the Controls/TNFi- (Over-represented by psoriasis patients) • Opportunistic infections were more common among the Cases/TNFi+ (p=0.08) • Nearly 40% of IMID/SIE treated patients had no pathogen identified • There was no significant difference in the number of Gram (+), Gram (-), and polymicrobic infections between the two groups • Opportunistic infx (MTb, Histoplasma) were only seen in TNFi + pts. • No psoriasis patients were seen in the Cases/TNFi+ • Infliximab was over-represented in the TNFi+ group • More Cases/TNFi+ receivd DMARDs and MTX • Drug use was otherwise the same between groups •
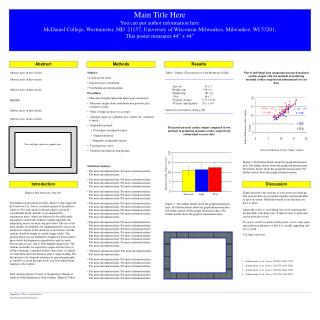
FULL ABSTRACT HERE PURPOSE: TNF inhibitors may increase the risk of SIE. Past studies have not documented the range and severity of TNFi SIE. This study reviews the scope of TNFi SIE from one institution. METHODS: Immune mediated inflammatory diseases (IMID) patients hospitalized between 1999-2006 for SIE were found by computerized searches of hospital records by cross-referencing discharge diagnoses (rheumatoid arthritis (RA), Crohn’s (CD), ankylosing spondylitis (AS), psoriatic arthritis (PsA) and psoriasis) with any of 18 SIE (e.g. pneumonia, septic arthritis, prosthetic infection, cellulitis, sepsis, tuberculosis). Two IMID groups were compared, those receiving TNFi (cases) and those not on TNFi (controls) at admission. The TNFi- control group included 2 age-matched patients for each TNFi+ patient. Only SIE related hospitalized patients with a reviewable chart were included. From 303 patients, we identified 41 patients receiving TNFi on admission. RESULTS. We examined 240 RA, 7 AS, 28 CD, 4 PsA and 24 psoriasis patients to find 41 TNFi+ SIE patients and 82 age-matched TNFi- controls. The 2 groups were matched for their age, gender, disease duration, and related IMID; with RA being most common (83% vs. 73%). Among TNFi+, more received infliximab (59%) than etanercept (29%) or adalimumab (12%). Prednisone use (46 vs 33%), dose (11.7 vs 7.7mg) and DMARD use (56% vs 32%) were greater in TNFi+ patients (p<0.05). Overall SIEs were the same between groups (Table). Similar organisms were cultured from TNFi+ vs TNFi- patients including S. aureus (14% vs 9%), MRSA (6% vs 7%), other Staph species (0% vs 4%), E. coli (10% vs 12%), S. pneumoniae (6% vs 1%) and other Strep (4% vs 3%). There was one death on each group due to pneumonia. TNFi+ patients trended towards more SIE complications (bacteremia, sepsis, abscess, osteomyelitis) (39% vs 29%) and longer hospitalizations (8.9 vs 6.5 days, p=0.08). CONCLUSIONS: This retrospective case control study did not show an increase in overall SIE attributable to TNFi use, but did show a small increased risk of opportunistic (2 Mycobacterial, 1 Histoplasma) and bone/joint infections compared with TNFi- IMID patients. SIE severity was greater in TNFi+ patients, with longer hospitalizations and more complications.
FULL ABSTRACT HERE PURPOSE: TNF inhibitors may increase the risk of SIE. Past studies have not documented the range and severity of TNFi SIE. This study reviews the scope of TNFi SIE from one institution. METHODS: Immune mediated inflammatory diseases (IMID) patients hospitalized between 1999-2006 for SIE were found by computerized searches of hospital records by cross-referencing discharge diagnoses (rheumatoid arthritis (RA), Crohn’s (CD), ankylosing spondylitis (AS), psoriatic arthritis (PsA) and psoriasis) with any of 18 SIE (e.g. pneumonia, septic arthritis, prosthetic infection, cellulitis, sepsis, tuberculosis). Two IMID groups were compared, those receiving TNFi (cases) and those not on TNFi (controls) at admission. The TNFi- control group included 2 age-matched patients for each TNFi+ patient. Only SIE related hospitalized patients with a reviewable chart were included. From 303 patients, we identified 41 patients receiving TNFi on admission. RESULTS. We examined 240 RA, 7 AS, 28 CD, 4 PsA and 24 psoriasis patients to find 41 TNFi+ SIE patients and 82 age-matched TNFi- controls. The 2 groups were matched for their age, gender, disease duration, and related IMID; with RA being most common (83% vs. 73%). Among TNFi+, more received infliximab (59%) than etanercept (29%) or adalimumab (12%). Prednisone use (46 vs 33%), dose (11.7 vs 7.7mg) and DMARD use (56% vs 32%) were greater in TNFi+ patients (p<0.05). Overall SIEs were the same between groups (Table). Similar organisms were cultured from TNFi+ vs TNFi- patients including S. aureus (14% vs 9%), MRSA (6% vs 7%), other Staph species (0% vs 4%), E. coli (10% vs 12%), S. pneumoniae (6% vs 1%) and other Strep (4% vs 3%). There was one death on each group due to pneumonia. TNFi+ patients trended towards more SIE complications (bacteremia, sepsis, abscess, osteomyelitis) (39% vs 29%) and longer hospitalizations (8.9 vs 6.5 days, p=0.08). CONCLUSIONS: This retrospective case control study did not show an increase in overall SIE attributable to TNFi use, but did show a small increased risk of opportunistic (2 Mycobacterial, 1 Histoplasma) and bone/joint infections compared with TNFi- IMID patients. SIE severity was greater in TNFi+ patients, with longer hospitalizations and more complications.
INTRODUCTION • Tumor necrosis factor (TNF) plays a pivotal role in immune-mediated inflammatory diseases (IMIDs), such as rheumatoid arthritis (RA), Crohn’s disease (CD), psoriasis and ankylosing spondylitis (AS). • TNF inhibitors (TNFi) have revolutionized the treatment of IMIDs. To date, >1.3 million patientsworldwide have received infliximab, etanercept, and adalimumab. • The versatile and pervasive role of TNF in host defense makes its therapeutic inhibition potentially tenuous, as TNF antagonism may increase the risk of serious infectious events (SIEs). Drug trials have shown SIE rates to be equal in placebo and TNFi treated patients. While some studies show no increase, others show higher rates of SIE in patients receiving TNFi. Nevertheless, there is limited data regarding the scope and severity of SIE in TNFi-treated patients. • We performed a retrospective chart review of TNFi-treated (TNFi+) & TNFi-naïve (TNFi-) IMID patients hospitalized for SIEs.
METHODS • Study subjects were identified by a computerized search of hospital discharge diagnoses and consultation records from the Infectious Disease Division between January 2000 and August 2006. We identified IMID patients hospitalized for an SIE. • IMIDs included ankylosing spondylitis (AS), Crohn’s (CD), psoriasis, psoriatic arthritis (PsA) and rheumatoid arthritis (RA). • Prespecified hospitalizable serious infectious events (SIE) included: abscess, cellulitis, encephalitis, endocarditis, histoplasmosis, influenza, listeria, meningitis, mycobacteria, osteomyelitis, pneumonia, pyelonephritis, sepsis, septic arthritis, septic prosthetic joint infection, tuberculosis, urinary tract infection or urosepsis. Outpatient SIEs were excluded from these analyses.
Only SIE-related hospitalized IMID patients with a reviewable chart were included. Each medical record was examined using a standardized template to document patient demographics, IMID diagnosis, type of infection (e.g. pneumonia, sepsis), organism, site of infection, severity, comorbidities, concurrent drug use (e.g. TNFi, DMARDs, steroids), outcomes, length of stay and recurrence. • 303 potential candidates were identified electronically. From this cohort we identified 41 IMID patients (13.5%) receiving TNFi (TNFi+) at the time of their SIE hospitalization. These are our index “CASES”. The “CONTROL” group consisted of two age- and gender- matched patients that were randomly chosen from the non-TNFi (TNFi-) patients. • This study was approved by the PHD institutional review board.
Can we compare the gram negatives between those on/not on TNF? Gram negs include E. Coli, haemophilus, prevotella, bacteroides, klebsiella, moraxella, pseudomonas
SUMMARY • This retrospective case-controlled study examined the types of Serious Infectious Events and related pathogens in TNFi treated immune mediated inflammatory disease patients. • Opportunistic infections were only seen in patients receiving TNF inhibitor therapy (Cases). • Cellulitis was significantly more common in the Controls (those not receiving TNF inhibitor therapy). • TNF inhibitor treated patients tended to have a longer length of hospitalization and more complications (ns).
CONCLUSIONS • This retrospective case-controlled study examined the types of Serious Infectious Events and related pathogens in TNFi treated immune mediated inflammatory disease patients. • Opportunistic infections were only seen in patients receiving TNF inhibitor therapy (Cases). • Cellulitis was significantly more common in the Controls (those not receiving TNF inhibitor therapy). • TNF inhibitor treated patients tended to have a longer length of hospitalization and more complications (ns).