
C-Reactive Protein
E N D
Presentation Transcript
Rosuvastatin to Prevent Vascular Events in Men and Womenwith Elevated C-Reactive ProteinPaul M Ridker, M.D., Eleanor Danielson, M.I.A., Francisco A.H. Fonseca, M.D., et al. for the JUPITER Study Group(Justification for the Use of Statins in Primary Prevention: an Interventional Trial Evaluating Rosuvastatin)The New England Journal of MedicineNovember 20th, 2008Journal ClubTatyana Danilov November 21st, 2008
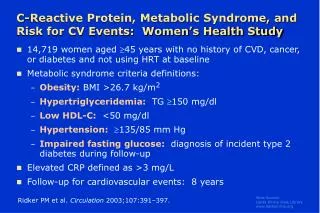
CRP and Cardiovascular Risk • Several large prospective epidemiological studies have shown that hs-CRP is a strong and independent predictor of cardiovascular disease • Incidence of first cardiovascular event • Long term risk of MI • Recurrence of vascular events • Ischemic stroke, PVD, sudden death, all cause mortality • CRP correlates with traditional risk factors • Correlation persists after adjustment for traditional risk factors • Highest CRP in patients with increased number of risk factors
Screening CRP • Hs-CRP levels • <1 mg/liter low risk • 1 to 3 mg/liter intermediate risk • >3 mg/liter high risk • >10 search for other inflammatory source • Two values measured 2 weeks apart • Recommended for intermediate risk patients if the result will change management • Universal screening currently not recommended
Statins and CRP • Statin therapy lowers CRP levels by 15-50% • Intensive statin therapy associated with greater reduction • Decrease in CRP independent of LDL reduction • Reduction in IL-6, TNF • Direct gene suppression • PROVE IT-TIMI 22 • Levels of hsCRP <2 mg/liter was as important for long-term event-free survival as was achieving levels of LDL cholesterol <70 mg/dl • Best long-term outcomes were found in those who achieved both these goals
Hypothesis/Objective • Healthy individuals with low-normal LDL levels and elevated CRP levels may benefit from statin therapy • To investigate the effect of treatment with Rosuvastatin 20 mg vs. Placebo on the rate of first cardiovascular events
Methods • Randomized, double-blind, placebo controlled, multicenter trial • 1315 sites, 26 countries • Financially supported by Astra-Zeneca (collected the trial data and monitored the study sites but played no role in the analysis of data)
Study Population Men 50 or older and women 60 or older without a history of cardiovascular disease AND At initial screening LDL cholesterol < 130 mg per deciliter (3.4 mmol per liter) AND high-sensitivity C-reactive protein level of ≥ 2.0 mg per liter.
Exclusion Criteria • previous or current use of lipid-lowering therapy • current use of postmenopausal HRT • hepatic dysfunction (ALT > 2x ULN), CK > 3x ULN • Cr >2 • Diabetes • Uncontrolled hypertension (>190 /100 mm Hg), • Cancer within 5 years • Uncontrolled hypothyroidism (TSH > 1.5 x ULN) • Recent history of alcohol or drug abuse • Patients with inflammatory conditions such as severe arthritis, lupus, or inflammatory bowel disease • Patients taking immunosuppressant agents (cyclosporine, tacrolimus, azathioprine, or glucocorticoids)
Methods • 4-week run-in phase during which all participants received placebo • Subjects randomly assigned in a 1:1 ratio to rosuvastatin, 20 mg daily or placebo • Follow-up visits scheduled at 13 weeks, then 6 months, then every 6 months until 60 months
End Points • Primary outcome was the occurrence of a first major cardiovascular event • Nonfatal myocardial infarction • Nonfatal stroke • Hospitalization for unstable angina • Arterial revascularization procedure • Confirmed death from cardiovascular causes • Secondary end point: death from any cause
Statistical Analysis • Event-driven trial • Statistical power of 90% to detect a 25% reduction in the rate of the primary end point • Two-sided significance level of 0.05 • All primary analyses were performed on an intention-to-treat basis • Cox proportional-hazards models were used to calculate hazard ratios and 95% C.I. for the comparison of event rates in the two groups • March 29, 2008, the independent data and safety monitoring board voted to terminate the trial – the stopping boundary was crossed at the first prespecified efficacy evaluation • Adverse-event reporting in a blinded manner continued until each participant had a formal closeout visit and discontinued therapy.
Results • 89,890 people were screened for enrollment between February 4th, 2003 to December 15th, 2006. • 72,088 were ineligible • 37,611 (52.2%) with LDL cholesterol levels ≥130 mg per deciliter • 25,993 (36.1%) with high-sensitivity C-reactive protein level less than 2.0 mg per liter. • A total of 17,802 people were randomly assigned to a study group
Table 1. Baseline Characteristics of the Trial Participants, According to Study Group
Kaplan–Meier Estimates NNT to prevent one primary outcome based on treatment with Rosuvastatin for 2 years is 95 NNT for 4 years is 31 NNT projected to 5 years is 25
Adverse Events Number Needed to Harm 166
Strengths • Large randomized double bind controlled trial – over 17 thousand patients • Diverse study population • Hard end points
Limitations • Early termination of study at less than 2 years • Safety of very low LDL • Safety of long term statin use • No subgroup analysis by CRP level • Do patients with a higher CRP account for most of the benefit? • Does not answer the question if CRP should be used as a general screening test for CAD • Did not compare patients with and without CRP measurements
A few weeks prior…New England Journal Article • A study of people with genetic variants of CRP assessed the effects of lifelong, persistently elevated CRP on ischemic vascular disease independent of other risk factors • CRP polymorphisms with high CRP levels were NOT associated with an increase in ischemic heart disease or cerebrovascular disease • Suggests that the increased risk of elevated CRP levels may not be causal but rather a marker of underlying atherosclerosis
Implications/Discussion • Who should be screened for elevated CRP levels? • Baseline level on all healthy patients along with baseline cholesterol • vs. continue to restrict to intermediate risk population • How often to repeat testing? • Will you change your practice based on this trial? • Earlier initiation of statin therapy • Lifestyle modification • Generally healthy study population • Absolute risk reduction is small 1.8% 0.9% • Large NNT • Cost effectiveness
Future… • Long term complications/side effects of prolonged high dose statin therapy • CRP targets for therapy • Better mechanistic understanding of CRP and vascular disease • Direct CRP inhibitors • Further studies are needed to identify novel vascular inflammatory markers and treatments