Kidney 1
Kidney 1. Renal Functions. Regulate volume/composition of extracellular fluid Contribute to acid/base balance by modulating excretion of fixed acids (i.e. anything but CO 2 ). Excretion of metabolites and foreign substances

Kidney 1
E N D
Presentation Transcript
Renal Functions • Regulate volume/composition of extracellular fluid • Contribute to acid/base balance by modulating excretion of fixed acids (i.e. anything but CO2). • Excretion of metabolites and foreign substances • Endocrine functions: secretion of renin and erythropoietin; conversion of calcitriol (Vitamin D) to active or inactive forms.
The concept of renal clearance • Clearance of a solute X is the volume of plasma totally cleared of that substance per unit time • Cx = ([X]urine)(Furine)/[X]plasma • For example, if [creatinine]plasma = 4 mg/liter, and • Total loss of creatinine in urine/day is 720 mg, then • The clearance of creatinine is 720mg/24 hr/4 mg/L = 180 liters/24 hours.
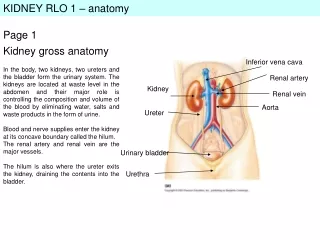
Gross Structure There are two basic types of nephrons: cortical or superficial ones with short Loops of Henle, and juxtamedullary ones with loops that descend into the inner medulla. In humans, only about 15% of the nephrons are juxtamedullary ones.
The nephron is the basic functional unit of the kidney The major parts of the nephron are Glomerulus Proximal tubule Loop of Henle Distal tubule Collecting duct
The first step in urine formation is glomerular filtration • Glomerular capillaries are 100X more leaky than ordinary capillaries • Glomerular filtrate contains all of the small solutes of plasma, but much less protein. • The driving force for glomerular filtration falls from about 17 mmHg at the head of the glomerular capillary bed to about 8 mmHg at the tail end – this is mostly due to an increasing concentration of plasma proteins.
The actual filter is the basement membrane of the glomerular capillary
Glomerular Filtration Rate • GFR is typically 90-140 ml/min in adult males, 80-125 ml/min in adult females. Or roughly 180 liters/day. • Of total renal plasma flow RPF, 20-25% gets filtered – this is the filtered fraction FF. • So, FF=GFR/RPF • Therefore, if cardiac output is about 7,200 liters/day, RPF is about 900 liters/day, and total renal blood flow is about 1,800 liters/day.
Measurement of GFR • To measure GFR, a marker substance is chosen that is freely filtered across glomeruli and neither reabsorbed nor secreted in the subsequent segments of the nephron. • Classically the substance used in experimental physiology was inulin, a plant polysaccharide. This has to be injected. Clinically, creatinine is used, although there is a small secretory component, because it is normally present in the blood.
Clearance effects of reabsorption and secretion • If a substance is both filtered and reabsorbed, its clearance is less than GFR; if a substance is both filtered and secreted, its clearance is greater than GFR. • Typically, both water and Na+ handling by the kidney are characterized by high levels of reabsorption: 95-98% of filtered water and Na+ are reabsorbed.
Measurement of RPF • A marker substance is chosen that is both filtered and also so effectively secreted that essentially all plasma that passes through the kidney is cleared of the substance. • The substance classically used for these measurements is para-amino hippuric acid, a product of metabolism of aromatic amino acids. • Remember PAH clearance measures renal plasma flow, not the volume flow of whole blood. To get whole-blood flow, divide the PAH clearance by the hematocrit.
Secreted: PAH Organic acids and bases Thiamine Guanidine Penicillin Choline Sulfonamides H+ (exchanged for Na+) Reabsorbed: Na+ K+ Glucose L amino acids Some vitamins Ca++, PO43- About 2/3 of filtered water, driven by net solute uptake. Tubular fluid leaving the PT is isosmotic with plasma. Functions of the Proximal Tubule
The concepts of filtered load and tubular maximum (Tmax) The filtered load of a substance is the rate of delivery to the renal tubules of that substance. The tubular maximum is the maximum rate of reabsorption of that substance. For glucose is about 375 mg/min. If the filtered load exceeds this value, the additional glucose will “spill over” into the urine.
A thought question • What would be the relationship between plasma concentration and excretion rate for a substance that is both filtered and secreted?
The Loop of Henle and DCT: Independent regulation of salt and water excretion • A regulatory problem is posed by the fact that loss and gain of salt and water do not occur in an isosmotic way. • The combination of transport processes in the DCT and Loop of Henle allow the production of either concentrated or dilute urine depending on the homeostatic need. This is done by modulating the rates of reabsorption of salt and water independently.
What happens in the Loop of Henle • Tubular fluid enters the Loop at about 300 mOsM. • As the fluid passes through the thin descending limb of the Loop, it passes through regions of steadily ascending ISF concentration. • Because the thin descending limb is much more permeable to water than to salt, water leaves the tubule, concentrating NaCl within the tubule
Ascending the Loop • As the tubular fluid enters the thin ascending limb of the Loop, it passes into a part of the tubule that is much more permeable to salt than to water. NaCl diffuses out of the tubule, leaving water behind. • As the tubular fluid passes through the thick ascending limb, Na+, Cl- and K+ are actively reabsorbed by the NK2C cotransporter. • The tubular fluid leaves the Loop more dilute than it was when it entered. However, because of NaCl reabsorption, urea has replaced NaCl as the major solute.
So, how are we going to get a concentrated urine? • The Loop of Henle creates an osmotic driving force that can be used if necessary for water recovery and urine concentration. How does it do it? The key lies in the active reabsorption of NaCl in the thick ascending limb of the Loop of Henle and distal convoluted tubule, together with the loop shape of the nephron.
The Two-solute Hypothesis Permeability Properties Ascending thin limb Medullary ISF Collecting Duct urea urea urea urea NaCl NaCl NaCl NaCl H2O H2O H2O H2O
Driving Forces (remember that, along the way between ATL and CD, urea replaced NaCl as the major solute) ATL Medullary ISF Collecting Duct urea UREA UREA NaCl NaCl NaCl H2O H2O H2O H2O Imagine starting the situation with equal osmotic concentrations in each compartment. The two solute gradients would both tend to drive solute into the ISF. Water can follow, but only from the collecting duct. The collecting duct urine therefore becomes concentrated. Urea can reenter the thin ascending limb, so on the average, each urea molecule may circle around several times before being excreted, carrying a proportionate amount of water back into the renal ISF each time.
ADH could be thought of as the hormone of water conservation • To produce a concentrated urine and thus recover the maximum amount of water, a high collecting duct water permeability is required. This process is controlled by antidiuretic hormone (ADH; arginine vasopressin in humans), a posterior pituitary neuropeptide. • In the presence of adequate ADH, water channels (aquaporins) are inserted into the collecting duct plasma membranes, enabling CD urine to become osmotically concentrated. • In the absence of ADH, aquaporins are recovered into the interior of the CD cells, and the dilute urine that enters the collecting duct passes through without much further modification.