Download
1 / 42
420 likes | 440 Views
Learn about the methamphetamine issue, effects, and strategies to tackle it in Native American tribes. Understand the impact and methods for prevention and treatment in this comprehensive initiative.

E N D
The Indian Country Methamphetamine Initiative: Taking Interventions to Scale Association of American Indian Physicians 39th Annual Meeting R Dale Walker, MD Patricia Silk Walker, PhD Michelle Singer August 9, 2010 Santa Ana Pueblo, New Mexico
Native Communities Advisory Council / Steering Committee Education Opportunity, Research Mentorship One Sky Center Training, Consultation, Technical Assistance Excellence Tribal Leadership
Goals for Today • The methamphetamine problem • The methamphetamine initiative • The Mission: Going-to-Scale • ICMI Tribal Sites • General Approaches • Logic Models • Examples
The most widely used illicit drug in the world except for cannabis. Worldwide it is estimated there are over 42 million regular users compared to approximately 15 million heroin users and 10 million cocaine users Meth use is increasing and expanding! Scope of the Meth Problem Worldwide
What is methamphetamine? • A powerful stimulant drug, classified as a psychostimulant • A Schedule II drug (along with cocaine and several other drugs) under the Federal Controlled Substances Act • A highly addictive drug
Why do people use meth? • Initially, methamphetamine decreases fatigue and appetite, heightens attention, and increases activity and respiration, creating feelings of high energy. • Meth enables people to stay awake and be physically (also sexually) active for long periods. Source: National Institute on Drug Abuse. April 1998, Reprinted January 2002.Research Report Series: Methamphetamine Abuse and Addiction. www.nida.nih.gov/ResearchReports/methamph/methamph.html
How does meth work? • Methamphetamine releases large amounts of dopamine in the brain, causing feelings of pleasure and euphoria. Source: National Institute on Drug Abuse. April 1998, Reprinted January 2002.Research Report Series: Methamphetamine Abuse and Addiction. www.nida.nih.gov/ResearchReports/methamph/methamph.html • Withdrawal symptoms may include fatigue, depression, anxiety, paranoia, aggression, and an intense craving for more of the drug. In some cases, psychotic symptoms may persist for months or years following use. Source: Office of National Drug Control Policy. November 2003. Fact Sheet: Methamphetamine. www.whitehousedrugpolicy.gov/publications/factsht/methamph/
How is meth used? • Injecting or smoking methamphetamine produces a short but intense and pleasurable “rush.” • When taken orally or by snorting, meth causes a less intense but much longer-lasting high that persists for several hours. Source: National Institute on Drug Abuse. April 1998, Reprinted January 2002.Research Report Series: Methamphetamine Abuse and Addiction. www.nida.nih.gov/ResearchReports/methamph/methamph.html
Why is Meth so Devastating? • Cheap, readily available • Stimulates, gives intense pleasure • Damages the user’s brain • Paranoid, delusional thoughts • Depression when stop using • Craving overwhelmingly powerful • Brain healing takes up to 2 years • We are not familiar with treating it
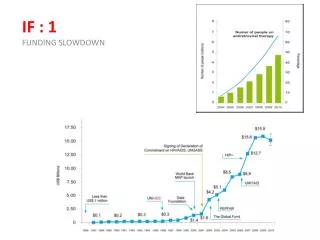
Young Adults (18 to 25) Reporting Past Year Methamphetamine Use: 2002 to 2005 Source: SAMHSA, 2002-2005 .
Methamphetamine Use in Past Year among Persons Aged >11, by Percentage and by Race/Ethnicity: 2002 - 2004 Percentage Source: SAMHSA 2004 NSDUH.
Methamphetamine Users (n= 1016) LIFETIME SUICIDE ATTEMPTS and BEHAVIOR PROBLEMS Zweben, et al., 2004
Clinical Challenges for Treatment of Methamphetamine Addiction • Poor treatment engagement rates • High dropout rates • Severe paranoia • High relapse rates • Ongoing episodes of psychosis • Severe craving • Protracted dysphoria Many patients may require medical/psychiatric supervision and need ongoing treatment with antipsychotic medications
“Tribal leaders unveil new meth Initiative”Indian Country Today • Create a National outreach campaign for all Native communities. • Establish and transfer community based, promising practices for prevention and treatment. • Work across Federal agencies for coordinated and consistent outreach strategy. NCAI President, Joe Garcia June 15, 2007
ICMI Partners Yakama Chippewa Cree Salt River San Carlos
An Ideal Intervention • Broadly based: Includes individual, family, community, tribe and society • Comprehensive: Prevention: Universal, Selective, Indicated Treatment Maintenance
Domains Influencing Drug Use Behavior: A Native Ecological Model Risk Protection Individual Peers/Family Community/Tribe Society/Cultural
Individual Intervention • Identify risk and protective factors counseling skill building improve coping support groups • Increase community awareness • Access to hotlines other help resources
Effective Family Intervention Strategies: Critical Role of Families • Parent training • Family skills training • Family in-home support • Family therapy Different types of family interventions are used to modify different risk and protective factors.
Community Driven/School Based Prevention Interventions • Public awareness and media campaigns • Youth Development Services • Social Interaction Skills Training Approaches • Mentoring Programs • Tutoring Programs • Rites of Passage Programs
Prevention ProgramsEnhance Protective Factors • strong family bonds • parental monitoring • parental involvement • success in school performance • pro social institutions (e.g. such as family, school, and religious organizations) • conventional norms about drug use
Prevention ProgramsReduce Risk Factors • ineffective parenting • chaotic home environment • lack of mutual attachments/nurturing • inappropriate behavior in the classroom • failure in school performance • poor social coping skills • affiliations with deviant peers • perceptions of approval of drug-using behaviors
Why Logic Models? • Logic models are useful • Clarification • Group work • Planning; project mgmt; evaluation • Logic models are required • Grant applications
Logic Model • Causes • Social Determinants • Risk and Protective Factors • Target Populations • Individuals; Families; Communities; Society • Approach/Strategy • Theory of Action • Manualized Activity and Materials Details • Outcomes (short; median; long)
Fighting Meth, Healing Families:Seven Promising Solutions 1. Media Campaigns 2. Expanding Permanency Options 3. Interagency Collaborations 4. New Supports for Grandfamilies 5. Enhancing Treatment Options 6. Family Drug Courts 7. Targeted Community Supports in Indian Country
ICMI Intervention Models • Community Mobilization • Capacity Development • Information • Treatment • Law Enforcement and Justice • Cultural Renaissance
Winnebago Tribe: Meth Task Force Goals and Objectives • Develop/maintain a Comprehensive Meth Prevention Strategy • Collectively plan and implement • Use Proactive measures • Use available funds - take immediate action • Working together to determine what fits • Broad based, multi-agency, systematic, family/community focused prevention- Community Mobilization
Dine Nation: What Works? • Community Education • Age-appropriate presentations, brochures, ads • Enforcement • Arrest and detainment for trafficking • Caring members of the community • Partnerships • Communities, chapters, private businesses and tribal divisions and programs • Capacity development. • Training for best, evidence based practice, integrated public health model. • Experienced at mobilizing communities across large area for interventions.
Northern Arapaho Tribe: a Comprehensive Systems Plan The Problem: • “turf” • gaps • duplications • crossed purposes Fragmented Service System The Solution: “Works” • client-centered • multi-agency • comprehensive • coordinated • Efficient • Implement Best Practice Treatment • 1. Information • 2. Multi-Systemic Family Therapy • 3. Critical Incident Counseling
Choctaw Nation of Oklahoma Adventure Therapy • “Natural Highs Program” • Transformation process • Experiential activities • Relationship building • Changing the way you live and think • Changing how you think and how you believe about life and yourself • Treatment. • Creation of challenge in a safe environment • Horses, Canoes, Tradition Camps
Meth Free Crow Walk: Youth as our Warriors in Reclaiming our Nation Meth Free Crowalition • Establish a “War Against Meth” Focus on accountability, prevention, intervention, and treatment • Combine forces for Unity. • Diverse community representation • Youth and Community Development: mentorship, leadership, trust, establish community norms. Law
Cultural Renaissance • All Sites
Effective Treatment Approaches For Methamphetamine Use Disorder • Motivational Interviewing • Therapeutic Use of Urine Testing • Contingency Management ( motivational incentive based) • Cognitive Behavioral Therapy - CBT • Community Reinforcement Approach • Matrix Model (combination of above)
Partnered Collaboration State/Federal Community-Based Organizations Grassroots Groups Research-Education-Treatment
Problem is bigger, broader and more complex than current solutions • Broad-based, integrated, interagency changes are needed. • State, county, and city relationships to be developed with tribes and communities • Training and tribal leadership development. • A Marshall Plan for all Native America that effects: economics, housing, social services, education, law/governance, and health.
Six Key PrinciplesEvidence-based predictors of change • Leadership • Mobilization Community driven • Public health approach • Strength based • Culturally informed • Proactive
Contact us at 503-494-3703 E-mail Dale Walker, MD onesky@ohsu.edu Or visit our website: www.oneskycenter.org
How to Use the Toolkit • Leadership and decision making • Overview of each module • Specific topics, issue pages • Promising Practice approaches • What the culture and science says • Training, technical assistance, and consultation • Reference documents • Toolkit webpage
Toolkit Essentials • Leadership Information • Methamphetamine Basics • Tribal Code-Policy • Media • Educational Materials and Presentations Prevention and Treatment Educational for Students, Parents, Community • Community Organizing • Fun Youth Items • Additional Resources