Cardiac
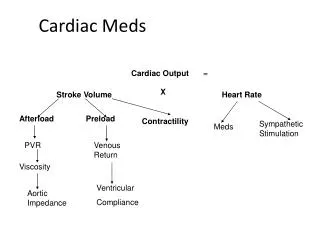
Cardiac. Elisa A. Mancuso RNC, MS, FNS Professor of Nursing. Hemodynamics. Preload - Venous return during diastole. Volume of blood = Hydration status Afterload - Arterial flow during systole. L Ventricular pressure to open Aortic valve. Cardiac Output = HR x SV

Cardiac
E N D
Presentation Transcript
Cardiac Elisa A. Mancuso RNC, MS, FNS Professor of Nursing
Hemodynamics Preload- • Venous return during diastole. • Volume of blood = Hydration status Afterload- • Arterial flow during systole. • L Ventricular pressure to open Aortic valve. Cardiac Output = HR x SV • Heart Rate X Stroke Volume
Murmurs Abnormal heart sounds • Improper closing or opening of valves • 80% of murmurs in kids are innocent • Close proximity of heart to chest wall • Stills Murmur– • Blood rushing out of aorta • Anemia • Fever
Fetal Circulation Oxygenated blood → Inferior Vena Cava (IVC) IVC → RA → FO → LA → LV → Aorta → Head & Arms • ↑↑ pressure inRA→Foramen Ovale (FO) • Bypasses the lungs and blood shunted to LA ↓ Blood returned → Superior Vena Cava (SVC) SVC → RA → RV → PA→DA →Aorta → Lower Body & Legs Ductus Arteriosus (DA) • Bypasses the lungs (↑↑ Pressure) • Only small portion of blood goes to pulmonary system • Blood gets re-oxygenated via placenta Ductus Venosis • Bypasses the liver and shunts blood to IVC
Fetal to Neonatal Circulation At birth lungs expand: • ↑O2 causes pulmonary vasodilation • ↓ Pulmonary pressure(resistance) • ↑Systemic pressure (resistance) • LA pressure > RA pressure • Foramen Ovalecloses within 1st hour of life • ↑O2 ↓Prostaglandins (from Placenta) • Ductus Arteriosuscloses within 10-24hours. • Permanent closure by 3-4 weeks. • PDA = Patent Ductus Arteriosus • In some cases can stay open for 3 months
Neonatal Circulation • Blood flows from higher to lower pressure • Systemic Pressure > Pulmonary Pressure L side > R side Blood flows from L → R side
Acyanotic Defects • L →R side shunt of oxygenated blood • ↑ Pulmonary blood flow • Pulmonary congestion • Heart is ineffective pump • Children prone to CHF • Prophylactic administration of antibiotics needed
Patent Ductus Arteriosus (PDA) Opening between the pulmonary artery (PA) and Aorta Oxygenated blood shunted from Aorta →→PA • ↑↑ Systemic resistance • Blood shunted to LA → LV → PA • ↑↑ Pulmonary Congestion • ↑↑ Back up to LA & LV • LV Hypertrophy
PDA Clinical signs • Soft - harsh systolic newborn murmur • Machinery type systolic and diastolic murmur in older children • ↑ RR & moist Breath sounds • Bounding pulses • ↑ HR • Widened pulse pressure • Large difference between the systolic • and diastolic pressure
Therapy • Indomethacin (indocin) • Prostaglandin inhibitor promotes vasoconstriction and closure of PDA • 3 Dose maximum q 12 hours • Ligation of Ductus Arteriosus • Close connection to prevent return of oxygenated blood to lungs • No open heart surgery
Atrial Septal Defect (ASD) Abnormal opening between the RA & LA • Blood flows from ↑↑press LA to ↓↓press RA • ↑↑ blood volume to right side of heart • Leads to RA and RV hypertrophy • ↑↑ blood volume to lungs • Pulmonary Congestion • DOE/ CHF symptoms • Crescendo/decrescendo systolic • ejection murmur
ASD Therapy • ASO (Amplatzer Septal Occluder) • via cardiac cath • Medications for CHF • Open heart surgery and bypass, performed before school age • Dacron patch • Low mortality rate
Ventricular Septal Defect (VSD) Abnormal opening between RV and LV • ↑↑O2 blood from LV to RV • ↑↑ blood to RV = RV hypertrophy • ↑↑ pulmonary flow • ↓↓ systemic flow • Spontaneous closure in 20%-60% within first year of life.
VSD Clinical signs • CHF = ↓↓CO, ↑HR, ↑RR, scalp sweating, • ↑ weight gain, irritability • Pulmonary edema • DOE, fatigue, ↓↓ PO intake • ↓↓Aorta Blood Flow • ↓↓ femoral and brachial pulses • ↓↓ BP x 4 • Harsh holosystolic murmur with thrill Therapy same as ASD
Pulmonic Stenosis (PS) Narrowing of the pulmonary valve • ↑↑ PA pressure/resistance • ↓↓ Pulmonary Blood Flow • Blood backs up into RV RV Hypertrophy
Clinical Signs & Therapy • Depends on size of stenosis • Pale, lethargic, slow feeder • Systolic ejection murmur • EKG and CXR show RV Hypertrophy Therapy • Pulmonary Valvotomy • Angioplasty • Enlarges ↑ pulmonic valve opening
Aortic Valvular Stenosis Narrowing of aortic valve • ↑↑ Resistance to blood flow from LV • causing LV Hypertrophy • ↑↑ back-up of blood in pulmonary system • ↑↑ Pulmonary congestion • ↓↓ blood via aorta ↓↓Systemic perfusion = ↓↓ CO
Clinical • Faint peripheral pulses RT ↓↓ CO • ↓↓ pulse pressure • Chest pain RT myocardial ischemia • Systolic ejection murmur Therapy • Commissurotomy • Enlarge aortic valve opening via angioplasty. • Additional surgery may be needed • later.
Coarctation of the Aorta • Narrowing of the aorta right after arch • ↑↑Pressure proximal to narrowing • ↑↑ BP upper body, arms & head • Bounding pulses & warm, ruddy skin • JVD • ↓↓Pressure distal to narrowing • ↓↓ BP lower body & legs • Weak pulses & cool, pale skin • Difference of 20mm for systolic BP
Clinical signs • ↑↑ BP in arms ↓↓ BP legs • Weak or Absent femoral pulses • Headache, blurred vision and nose bleeds • ↑↑risk for stroke • Older kids leg pain on exertion RT ↓ blood Therapy • Prostaglandin E – keep PDA open • Surgery • Resect coarcted portion and reanastomosis
Cyanotic defects • Unoxygenated blood enters systemic system • “Right to Left shunt” (R→ L) • Blood is shunted from venous to arterial • ↑↑ CHF and hypoxic episodes Now classified as: ↓↓ Pulmonary blood flow or Mixed blood flow defects
Transposition of Great Vessels (TGA) • Two separate circulations! • Aorta arises from RV • Unoxygenated blood enters aorta →Systemic • Pulmonary artery (PA) arises from LV • Oxygenated blood enters PA → recycled lungs → Pulmonary veins → LA No Oxygenated blood in systemic circulation!
TGA CLINICAL SIGNS Depends on type and size of associated defects • Severely cyanotic at birth • minimal communication between 2 systems • Large septal defects or PDA • Less cyanotic but may have CHF symptoms • ↑↑ HR, ↑↑ RR and cardiomegaly • Fatigue when feeding • ↓↓ Intake • ↓↓Output = Edema
THERAPY Prostaglandin E1 (Prostin VR or Alprostadil) • Vasodilator • Relaxes smooth muscle of ductus arteriosus • Keeps PDA open • Provides mixing of oxygenated and deoxygenated blood to systemic circulation. “Rashkind procedure” • Cardiac cath to create ASD • Maintains mixing of blood • Arterial switch procedure usually performed • in first few weeks of life
Tetralogy of Fallot Involves four cardiac defects • VSD • Blood shunted RV→ LV • Pulmonary Stenosis • ↓↓ blood to PA • Overriding Aorta • Sits over VSD • RV Hypertrophy • ↑ pressure from stenosis
Clinical signs of Tetralogy • First cry hypoxic and cyanotic • ↑↑ Activity = ↑↑ Hypoxia and ↑↑ Cyanosis • Pulse oximeter in low 70’s • ↑↑ Pulmonary stenosis = ↑↑ Cyanosis • ↑↑ HR, ↑↑ RR • Tire easily can’t finish feedings = ↓↓ Intake • Chronic O2 deficit → Polycythemia • ↑↑ # RBC’s to supply 02 to body • ↑↑Risk of CVA or embolism with dehydration
Clinical Manifestations • “Tet” Spells • ↑↑ Activity or ↑↑ Crying = ↓↓ blood flow to brain • ↑↑ hypoxia, cyanosis and fainting • Squatting • compensatory action • Knee chest position • ↓↓femoral blood flow ↑↑blood flow upper body • Clubbed fingers • Mental retardation
Therapy • Prostaglandin E1 • Maintain PDA • ↑↑ Pulmonary perfusion • Surgery • Patch the VSD • Open stenotic pulmonary valve • Heart Transplant with severe defects
Hypoplastic Left Heart (HLHS) Fatal anomaly • Non-functioning LV • Severe Aortic Stenosis • ASD • Aortic valve and Mitral valve Atresia • PDA • Clinical Signs • ↓↓ systemic output • ↓↓ B/P • ↓↓ Perfusion • Faint, weak pulses (<+1)
Treatment • ExtraCorporal Membrane Oxygenation (ECMO) • ↑↑ Risks & Costs ($250,000/day) • ↓↓ Availability @ Regional centers • Heart Transplant • ↓↓ Donor hearts • 3 Stage surgery if child can tolerate it. • DNR & Letting Go • Bereavement
Tricuspid Atresia (TA) Three major defects • No tricuspid valve • ASD & VSD • RV Hypoplasia Lungs receive blood via • PDA • small VSD • bronchial vessels • As long DA remains open the child • receives adequate O2.
Clinical Signs • Cyanosis • ↑↑ HR ↑↑ RR • Dyspnea with activity • Systolic murmur • Squatting • Polycythemia • Clubbed fingers
Therapy • Prostagladin E • Maintain PDA for 2 weeks then need surgery. • Surgery- • Anastomosis to allow blood flow to lungs. Three stages • Blalock-Taussing @ 2 weeks of age shunt btwn PA and Aorta • Glenn @ 6 month to a year shunt from SVC to PA to lungs 3)Fontan @ 2-3 years shunt from IVC to PA to lungs No more mixing of blood
Truncus Arteriosus • One common artery arises from LV & RV. • Overrides a large VSD • No separate PA or Aorta • Unoxygenated blood enters systemic circulation • ↑↑ blood volume flows to lungs • ↑↑ pulmonary blood flow • ↑↑ pulmonary edema ↑↑ CHF
Treatments • CHF and fluid overload • Lasix (1 mg/kg/dose) • Diurectic = ↓↓ edema ↓↓ Na, ↓↓ K+ • Digoxin (Digitalization Dosing) • Cardiac glycoside = ↓↓ edema • Surgery • VSD • R side graft
Nursing Interventions • √ Maternal History: • Rubella, DM, ETOH or Cardiac disease • Congenital heart disease • Chronic maternal illness • Perinatal infections (TORCH) • ertain meds maybe linked • Substance Abuse • ETOH may be associated with FAS andTetralogy of Fallot
Physical Exam Thoracic Exam Cardiac Sounds • √ Location of PMI (5th LICS MCL) • √ Rate • √ Rhythm • √ Murmurs • location, intensity and where in cardiac & respiratory cycles • √ visible pulsation on thorax • √ JVD Breath Sounds • √ Rate, rhythm • √ Dyspnea and Grunting (keep alveoli open) • √ Adventitious sounds • Moist- Pulmonary congestion or CHF
COLOR • √Mucous membranes • Lips, conjunctiva and nail beds. • √ Cyanosis • @ rest or with activity • √ clubbed fingers • Flushed cheeks = Polycythemia • KEEP INFANTS HYDRATED! • WHY?
Pulses • Palpate bilaterally • Compare upper and lower extremities • Absent or ↡femoral pulses in Coarctation • √ Rate/Rhythm/strength (0-+4) • √ BP all four extremities • Widened pulse pressure in PDA • ↑↑ BP upper extremities in Coarctation.
Nutritional Status √ Intake • Rest periods needed? • Time needed to complete feedings • ↓↓ intake, tiring due to ↓↓ available O2 √ HT, WT and HC √ Activity level-tires easily? • Developmental tasks achieved?
Respiratory Infections ↑↑Risk • Pulmonary vascular congestion • Bacterial invasion and growth • RT stasis of secretions (prophylaxis meds) Therapy • Meds • Bronchodilators • Steroids • PD & C • O2
Compensatory Mechanisms • Cardiomegaly • ↑ pumping action of heart = ↑ SV • ↑ use of cardiac muscle = ↑ O2 availability • ↑ size = hypertrophy • Tachycardia>160 in infant • ↑ rate = ↑ CO • ↑ O2 to tissues and vital organs • Polycythemia • ↑ production of RBC’s • ↑ availability of O2 to tissues • ↑ viscosity of blood • ↓↓ flow, sluggish • ↓↓ decreased peripheral circulation • High risk for CVA • Tachypnea> 60 in infants • ↑↑ RR = ↑↑ O2
Compensatory Posturing • ↑↑O2 to vital organs by ↓↓ workload of heart • Less area for blood to flow = ↓↓ venous return • “TET Spells” • Infants • May be flaccid with extremities extended • Knee chest position (infant seat) • Preschool • Squatting position • occludes femoral vein = ↓↓ venous return ↓↓ workload on heart ↑↑O2 sat & ↑↑ blood to vital organs
Congestive Heart Failure CHF Children’s CHF due to congenital heart defects • CHF = ↓↓ Contractility of heart = ↓↓ CO • ↓↓ blood volume for systemic circulation • ↑↑ pulmonary congestion • ↓↓ O2 and ↓↓ nutrition. Unable to meet metabolic demands
Interventions Parent teaching • Review defect and s/s when to call MD • Meds - dose, schedule, SE • Prophylactic antibiotics • Immunizations • Nutrition - ↑ cal formula, ↑ Fe, ↑ K+, ↑ Protein, ↓ fat, ↓ Na • Activity- allow for rest periods for fatigue • ↓ Cardiac demands • Position, thermoregulation • “Cardiac Cripple” • Parents overprotect and child manipulates Set limits & discipline WNL • Emotional support (access to NP/RN 24 hours) • Encourage support groups (specific to defect)
Medications Digoxin • Action -cardiac glycoside • ↑ Contactility of heart = ↑ efficacy = ↑ CO • Slows down SA node = ↓ HR • Digitalization Loading Dose = 30-40 mcg/kg/dose ÷ (½, ¼, ¼) Maintenance dose = 4-5 mcg/kg/day ÷ q 12 Nursing interventions √ Apical pulse for one full minute before giving med. Hold med if: Infant <100 Toddler <90 Preschool <70 School age <60 Document Apical HR next to dose on MAR
Nursing Interventions • √ I and O and √ K+ level • ↓↓ K+ = ↑↑ Dig toxicity • √ Serum Digoxin level (0.5-2ng/dl) • Digoxin Toxicity (>3ng/dl) • vomiting (earliest sign), nausea (↓↓ Po intake) • lethargy and bradycardia • Administer with 2 RN’s • Review order & √ HR parameters √ Dosage and calculation √ Actual dose in syringe a administering Document on MAR: HR & Initials @ dose
Diuretics Action- eliminates excess H2O and Na = ↑ fluid loss ↓edema and ↓work for heart and lungs • Furosimide-Lasix (Strong acting) 1mk/kg/dose • Blocks reabsorption of Na+ H2O @ loop of Henle • ↑↑↑ loss of Na+, K+ and H2O • Thiazides-Diuril 10-20 mg/kg/dose • Blocks reabsorption of Na+ H2O K+ distal tubules • ↑↑↑ loss of Na+, K+ and H2O • Aldactone (Aldosterone Inhibitor)- (K+ Sparing) • Blocks action of Aldosterone • hormone that retains Na+ and H2O Promotes H2O and Na+ loss &Retains K+
Nursing Interventions √ Weight • Same time, scale and amount of clothing = None! √ I and O • weigh all diapers • √ skin tugor on sternum (tenting= dehydrated) √ Serum electrolytes • K+, Na+, BUN and Creatine Administer K+ supplements KCL, Slo-K, K-Lor, K-Dur K+ level affects Digoxin efficacy!
Prostaglandin E1 (Prostin VR) Vasodilator (0.1 ug/kg/min) • Relaxes vascular smooth muscle • Keeps open Ductus Arteriosus (DA). • ↑ Pressure in L heart = ↑ pressure in Aorta • Blood shunted from Aorta ➔ PDA ➔ PA • ↑ Blood to lungs =↑ perfusion = ↑ oxygenation • ↑ O2 to systemic circulation Maintains mixing of oxygenated and deoxygenated blood in cyanotic defects.