Chapter 15 The Urinary System
Chapter 15 The Urinary System. Biology 112 Tri-County Technical College Pendleton, SC. Functions of Urinary System. Regulating blood volume and blood pressure adjusting volume of water lost in urine, releasing erythropoietin and renin

Chapter 15 The Urinary System
E N D
Presentation Transcript
Chapter 15 The Urinary System Biology 112 Tri-County Technical College Pendleton, SC
Functions of Urinary System • Regulating blood volume and blood pressure • adjusting volume of water lost in urine, releasing erythropoietin and renin • Regulating plasma [ ]s of Na+, K+, Cl-, and other ions by controlling quantities lost in urine and controlling Ca+2 ion levels by synthesis of calcitriol • Stabilizing blood pH by controlling loss of hydrogen ions and bicarbonate ions in urine
Functions, cont. • Conserving valuable nutrients while eliminating organic waste products, especially nitrogenous products like urea and uric acid • Assisting liver in detoxifying poisons and during starvation, deaminating amino acids so can broken down by other tissue • PERFORMS vital excretory functions and eliminates organic wastes generated by cells throughout the body
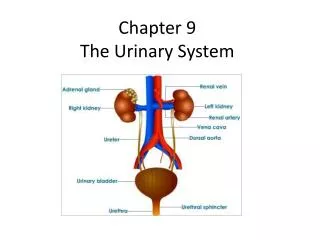
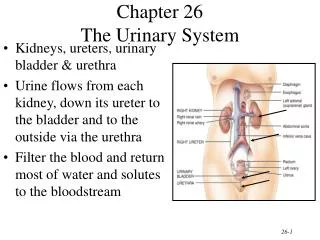
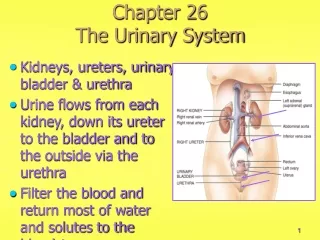
Location is everything…almost • Kidneys, ureters, urinary bladder, and urethra • Pair of kidneys located retroperitoneal (beneath parietal peritoneum) in superior lumbar region (T12-L3 vertebra) • Each kidney drained by ureter into urinary bladder located in lower pelvic region • Urinary bladder is drained by the urethra
Kidney Structure • Medial indention called HILUS where ureters, renal blood vessels, and nerves enter/exit the kidney • Renal cortex=outer layer (light colored) • Renal medulla=beneath cortex with many triangular regions (striped) which are the renal pyramids • Medulla is darker, reddish brown area • Broader base of each pyramid faces cortex with tip facing inner region of kidney • Pyramids separated by renal columns
Structure, cont. • Medial to hilus is flat, basinlike cavity called renal pelvis • Pelvis continuous with ureter leaving hilus • Extensions of the pelvis, the calyces (minor and major) form cup-shaped areas that enclose tips of the pyramids • Calyces collect urine with drains from tips of pyramids into renal pelvis • Urine flows from pelvis into ureterbladder for temporary storage
Nephron Structure • Are structural and functional unit of kidney • Responsible for urine production • Each nephron has 2 main structures—Glomerulus and Renal Tubule • Glomerulus is knot of capillaries • Renal tubule is cup-shaped and closed end completely surrounds glomerulus • Enlarged portion of renal tubule called GLOMERULAR (Bowman’s) CAPSULE
Nephron Structure, cont. • Inner layer of capsule composed of highly modified cells called podocytes • Podocytes have long branching processes that intertwine with each other and cling to glomerulus • Openings (slits) exist between extensions to form porous membrane around glomerulus • Rest of tubule coils and twists (Proximal) before forming hairpin curve (Loop of Henle) and then Distal Convoluted tubule before entering Collecting Duct
Nephron Structure, cont. • Glomerular capsuleproximal convoluted tubuleLoop of Henledistal convoluted tubulecollecting duct • All tubules cells have microvilli (proximal has the most) • Cortical nephrons most numerous—located almost entirely within cortex • Juxtamedullary nephrons-situated close to cortex-medulla junction and their loops of Henle extend deep into the medulla
Nephron Structure, cont. • Collecting ducts receive urine from many nephrons • Ducts run downward through medullary pyramids giving them a striped appearance • Collecting ducts deliver final urine product into the calyces and renal pelvis
Nephron Blood Flow • Every nephron associated with two capillary beds: glomerulus and peritubular capillary bed • Glomerulus fed and drained by arterioles • Afferent (from interlobular artery) is feeder vessel and efferent arteriole receives blood that has passed through the glomerulus • Glomerulus specialized for FILTRATION
Nephron Blood Flow, cont. • Afferent arteriole has larger diameter than efferent so BP in glomerulus very HIGH • This high pressure forces fluid and solutes (smaller than proteins) OUT of blood into glomerular capsule • Peritubular capillaries arise from efferent arteriole that drains glomerulus • These capillaires are LOW pressure porous vessels adapted for ABSORPTION rather than filtration
Nephron Blood Flow, cont. • Peritubular capillaries cling closely to whole length of renal tubule • Ideal position to receive solutes and water from tubule cells as these substances are “reabsorbed from filtrate moving through tubule • Peritubular capillaries drain into interlobular veins leaving the cortex
Processes of Urine Formation • Filtration, reabsorption, and secretion • FILTRATION is nonselective, passive process • Glomerulus acts as filter and filtrate formed essentially blood plasma w/o proteins • Blood proteins and blood cells too large to pass through filtration membrane • When either appear in urine=problem with glomerular filters
Urine Formation, cont. • Systemic BP normal, filtrate WILL be formed • Arterial BP < too low, glomerular pressure becomes inadequate to force substances out of blood into tubules and filtrate formation STOPS • Oliguria=abnormally low urinary output (100-400 ml/day) • Anuria=urine output < 100 ml/day • Low urine output=low blood pressure, transfusion reactions, acute inflammation, or crush injuries of kidneys
Reabsorption • Designed to reclaim useful substances • Filtrate contains wastes/excess ions that must be removed but also contains water, glucose, amino acids, and ions that must be reclaimed and returned to blood • Tubular reabsorption begins as soon as filtrate enters proximal convoluted tubule • Water by osmosis, most others by active transport • Uses membrane carriers and is VERY selective
Reabsorption, cont. • Carrier numbers are the KEY • Glucose & AAs completely retained and nitrogenous wastes almost completely excreted • Various ions reabsorbed/excreted to maintain proper pH/electrolyte balance of blood • Most reabsorption occurs in proximal tubules, but under certain conditions, distal CT/collecting duct also active
Secretion • Tubular secretion essentially reabsorption in reverse • H+; K+; and creatinine removed from blood and moved through tubule cells into filtrate • Absolutely essential for ridding body of substances NOT in filtrate (certain drugs) and as additional means of controlling pH
Nitrogenous Wastes • Most important are urea, uric acid, and creatinine • Urea product of deamination of AAs • Uric acid = nucleic acid metabolism • Tubule cells have few membrane carriers to reabsorb these substances and usually found in high [ ]s in urine • Creatinine actively secreted into filtrate
Water and Electrolyte Balance • Water occupies 3 main locations in body (fluid compartments) • Intracellular fluid (about 2/3 of body fluid) • Extracellular fluid (80% interstitial or tissue fluid and 20% is blood plasma) • More to fluid balance than just water-types and amounts of electrolytes (Na+, Ca++, K+) also very important to body homeostasis
Balance, cont. • Water and electrolyte balance linked as kidneys process blood • Body cannot afford to lose more water than it takes in • Most water intake is from fluids/foods consumed-about 10% comes from metabolism • Water leaves via vaporization from lungs, perspiration, and defecation
More Balancing… • Reabsorption of water/electrolytes by kidneys regulated primarily by hormones • Blood volume dropsBP dropsdecreases filtrate formedosmoreceptors in hypothalamus direct posterior pituitary to release ADH (kidney tubule cells) reabsorb more waterblood volume & BP increase • Only small amount of very [ ]ed urine produced
Balancing the balancing • ADH not released (injury/destruction of hypothalamus/posterior pituitary) huge amts of very dilute urine flush from body daily • Diabetes insipidus can lead to severe dehydration and electrolyte imbalance • Aldosterone (adrenal cortex) major factor regulating Na+ content of ECF and helps regulate [ ] of other ions (Cl-, K+, Mg++) • Secretion of aldosterone influenced by falling BP or low levels of Na+ in blood
OMG, more balancing… • Na+ MOST responsible for water flow • W/WO aldosterone, about 80% of Na+ in filtrate reabsorbed in proximal CT • If aldosterone [ ]s high, most of remaining Na+ reabsorbed in distal CT • Sodium chloride actually reabsorbed because Cl- follows Na+ • For each Na+ reabsorbed, a K+ is secreted into filtrate = back to normal balance in blood • As Na+ reclaimed, water follows passively
Please, no more balancing • Most important trigger for aldosterone release is renin-angiotensin mechanism • Juxtaglomerular apparatus (consists of modified smooth muscle cells in afferent arteriole + modified epithelial cells in part of DCT) stimulated by low BP or changes in solute content in filtraterelease renin into bloodcatalyzes production of antiotensin IIvasoconstriction of blood vessels and release of aldosterone by adrenal cortex cellsblood volume and BP >
The end of balancing..for now!! • Renin-angiotensin mechanism EXTREMELY important for regulating BP • Individuals with Addison’s disease (hypoaldosteronism) have polypuria • Excrete large volumes of urine and lose tremendous amounts of salt and water in urine
Acid-Base Blood Balance • Blood pH must be maintained ~ 7.35-7.45 • Alkalosis=pH above 7.45; acidosis= <7.35 • 7.35 represents higher than optimal H+ [ ] for functioning of most body cells • Any arterial pH between 7.35 and 7.00 called physiological acidosis • Small amounts of acidic substances in ingested foods but most H+s originate as by-products of cellular metabolismadds substances to blood that tend to disturb its acid-base balance
Not the same balancing… • Metabolism produces many acids (phosphoric, lactic, types of fatty acids) • Carbon dioxide released by metabolism forms carbonic acid • Cells also release ammonia and other basic substances as they go about their business • Blood buffers can tie up excess acids and bases (temporarily) and lungs have chief responsibility of eliminating carbon dioxide
Who is on first? • Kidneys assume most of load for acid-base balance of blood • Buffers first line of defense in resisting pH changes • Bicarbonate, phosphate, and protein buffer systems are 3 major buffer systems of body • All work essentially in the same way….
Bicarbonate Buffering • Mixture of carbonic acid (H2CO3) and its salt, sodium bicarbonate (NaHCO3) • Bicarbonate ion (HCO3-) act as base to tie up H+s if blood becoming acidic • Carbonic acid (H2CO3) dissociates in presence of rising OH- (blood becoming more basic) and releases H+s to bind with OH-s • Buffers can tie up excess acids/bases temporarily but CANNOT eliminate them from the body • Lungs can dispose of carbonic acid by eliminating carbon dioxide
Buffer me up…Scotty!!! • ONLY kidneys can rid body of other acids (from metabolism) and ONLY kidneys have power to regulate blood levels of alkaline substances • Most IMPORTANT for kidneys are excreting bicarbonate ions and by conserving (reabsorbing) or generating new bicarbonate ions
I Can’t Do It, Captain…. • Losing a HCO3- from body has same effect of gaining a H+ since it leaves a free hydrogen ion • Reabsorbing or generating an new HCO3- is same a losing a H+ because it tens to combine with a H+ • Urine pH ranges from 4.0 to 6.5 reflecting ability of renal tubules to excrete basic or acid ions to maintain blood pH homeostasis
The Urinary Bladder • Smooth, collapsible, muscular sac • Three openings: 2 ureter and 1 urethra (drains the bladder) • Smooth triangular region of bladder base outlined by three openings called the trigone (infections tend to persist in this region) • Bladder wall contains 3 layers of smooth muscle (detrusor muscle) and its mucosa is special type of epithelium called transitional epithelium
But Mommy, I really have to go.. • When empty, bladder is collapsed and its walls are thick and folded • Urine accumulates, its muscular walls stretch and transitional epithelium thins allowing bladder to store more urine w/o increasing its internal pressure • Urine formed continually by kidneys and usually stored in bladder until its release is convenient (or NOT)
Micturition • Act of emptying the bladder • Two sphincters (valves) control flow from bladder (internal and external urethral sphincter) • About 200 mls of urinestretch receptors activatedimpulses to sacral region of spinal cordback to bladder via pelvic splanchnic nervesbladder goes into reflex contractions
Micturition, cont. • Contractions force stored urine past internal sphincter (smooth muscle-involuntary) into upper part of urethra • Person feels urge to void • Lower external sphincter is skeletal muscle and subject to voluntary control so “going” can be delayed • Eventually, micturition occurs whether one wills it or not!!!
Some Key Terms • Incontinence occurs when one is unable to voluntarily control external sphincter • Normal in children less than 2 YOA; those who sleep too soundly, & emotional problems, pressure, and/or nervous system problems (stroke/spinal cord injury) • Retention is condition in which bladder is unable to expel contained urine • General anesthesia surgery; hypertrophy
Key Terms, cont. • Hypertrophy: enlargement of prostate gland which surrounds neck of bladder • Urethritis: inflammation of urethra • more common in females • Cystitis: inflammation of urinary bladder • Symptoms include dysuria, urinary urgency and frequency, fever, cloudy/blood-tinged urine • If kidneys involved; back pain and severe headache common
Key Terms, III • Escherichia coli normal flora of intestinal tract • pathogenic in sterile urinary tract • Glomerulonephritis: glomerular filters become clogged with antigen-antibody complexes resulting from streptococcal infections • Occurs most often in children with strep throat or scarlet fever that was not treated promptly or properly
Key Terms IV • Urgency describes feeling that it is necessary to void • Frequency describes frequent voiding of small amounts of urine • Both are generally consequences of aging process which causes bladder shrinkage and loss of bladder tone