Download
1 / 22
230 likes | 563 Views
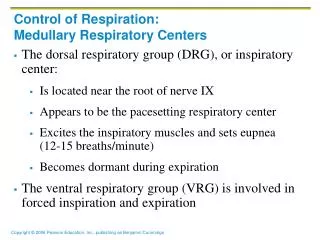
Control of Respiration Week 5. Dr. Walid Daoud A. Professor. Non-Chemical (Nervous) Regulation of Respiration. 1-Afferents from higher centers (Cerebral cortex) Voluntary Respiration: Example: talking, singing are controlled expiratory efforts and expiration occurs at the

E N D
Control of RespirationWeek 5 Dr. Walid Daoud A. Professor
Non-Chemical (Nervous) Regulation of Respiration 1-Afferents from higher centers (Cerebral cortex) Voluntary Respiration: Example: talking, singing are controlled expiratory efforts and expiration occurs at the end of each expiratory effort. Pathway: excitatory and inhibitory afferents pass from cortex to RC neuron in brain stem or bypass directly to spinal motor neuron of respiratory muscles.
Forms of Voluntary Respiration 1-Voluntary Hyperventilation: Its duration is limited by CO2 level in blood. When CO2 decreases, respiration stops for a while and is resumed again when CO2 accumulates and reaches its normal level.
Forms of Voluntary Respiration 2- Voluntary Apnea (Breath Holding): Voluntary stop of breathing e.g, swimming but after 45-60 sec. the person has desire to breathe (breaking point) due to decrease in arterial PO2 and increase in arterial PCO2. This causes chemical drive of respiration.
Voluntary breath holding can be prolonged by: 1-Initial hyperventilation before breath holding. 2-Prior inhalation of pure O2 for 1 min. 3-Hold breath in full inspiratory position. 4-Viscerel reflexes e.g, swallowing.
II-Afferent from Respiratory Mechanoreceptors 1- In upper respiratory passages: Irritant receptors: in resp. mucosa Stimulus: mechanical (dust, mucus, food) Response: -Cough. -Sneezing. -Bronchoconstriction.
Cough Reflex Stimulus: irritation, congestion, inflammation Receptors: free nerve endings of vagus. Afferents via vagus. Cough center: in medulla oblongata. Efferents to abdominal muscles which contract increasing intra-abdominal pressure.
Mechanics of Cough 1- Inspiratory phase. 2- Compressive phase. 3- Expiratory blast phase.
Sneezing Reflex Stimulus: irritation of nasal mucosa. Afferent to medulla via trigeminal nerve. Sneezing center in medulla. Efferent to expiratory muscles which contract with opened glottis.
II-Afferent from Respiratory Mechanoreceptors 2- Lung Stretch Receptors: Lung contains 2 types of receptors: . Slowly adapting receptors (SAR): stretch receptors. . Rapidly adapting receptors (RAR): - Irritant receptors. - J-receptors. Stimulated receptors send afferent impulses to RC in medulla via vagus. Hering-Breuer reflex
III-Afferent from chest wall receptors In chest wall muscle and their tendons Afferent to RC via vagus to inform about chest wall position and respiratory efforts Inhibit DRG to stop inspiration. These receptors determine tidal volume in human adults.
IV-Afferents from proprioceptors Afferents from skeletal muscles, tendons and ligaments during exercise. Stimulated by movement of muscles and joints. Causes reflex stimulation of ventilation.
V-Afferents from cardiovascular system 1-Arterial baroreceptors (high pressure receptors): in aortic arch and carotid sinus. 2-Atrial receptors (low pressure receptors): In right atrium and big veins
VI-Visceral reflexes 1- Swallowing. 2- Hiccup.
Hypoxia It is oxygen deficiency at tissue level. Types: 1- Hypoxic hypoxia. 2- Anemic hypoxia. 3- Stagnant hypoxia. 4- Histotoxic hypoxia.
Hypoxic hypoxia It is caused by inadequate oxygenation or decreased PO2 in arterial blood. Causes: 1- Low O2 tension in inspired air. 2- Pulmonary disorders: . Impaired ventilation. . Impaired perfusion. 3- Shunting of venous into arterial blood.
Anemic hypoxia It occurs when there is deficiency of Hb capable of carrying O2. Causes: 1- Insufficient Hb (anemias). 2- CO poisoning (carboxy-Hb).
Stagnant hypoxia It occurs due to inadequate blood flow to tissue or slow circulation. Causes: 1- Generalized. 2- Localized.
Histotoxic hypoxia It occurs when tissues can not utilize O2. Causes: 1- Cyanide poisoning. 2- Alcohol or narcotic poisoning.
Cyanosis It is bluish coloration of skin and mucous membranes due to presence of increased amount of reduced hemoglobin more than 5 grams / 100 ml capillary blood. Types: 1- Central. 2- Peripheral.
Cyanosis Causes: 1- hypoxic hypoxia. 2- stagnant hypoxia. 3- all causes of asphyxia.