Download
1 / 42
420 likes | 440 Views
Ensuring best management for rare diseases, focus on drug-resistant tuberculosis, multidrug-resistant rates highest ever. Proposal for coordinating national MDR-TB service for optimum treatment and outcomes. Challenges in implementation, ethical and political considerations.

E N D
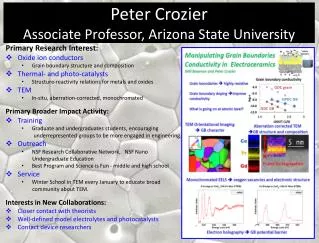
How can we ensure that patients with a rare disease get the best management? Drug resistant Tuberculosis shows a way • Professor Peter D.O.Davies, • Liverpool
Proportion of tuberculosis cases with first line drug resistance, UK, 2000-2007 First line drugs: isoniazid, rifampicin, ethambutol & pyrazinamide (except Mycobacterium bovis) Multi-drug resistant: resistant to isoniazid and rifampicin (with or without other resistance) Source: Enhanced Tuberculosis Surveillance (ETS), UK Mycobacterial Surveillance Network (MycobNet), Enhanced Surveillance of Mycobacterial Infections (ESMI) 02/10/2008
Multiple drug resistanceDOTS-Plus in Latvia Lemaine V et al. Lancet 2005; 365:318-26
WHO report 2008 26 FEBRUARY 2008 WASHINGTON DC /GENEVA • Multidrug-resistant tuberculosis (MDR-TB) has been recorded at the highest rates ever, according to a new report published today. • http://www.who.int/tb/publications/2008/drs_report4_26feb08.pdf
Warning • A new plague is sweeping across the planet • Soon multidrug resistant tuberculosis • will kill one person in three • The Constant Gardener November 2005
The management of MDRTB • A rare disease no national guidelines. • Little personal experience. • Scattered occurrence • What drugs and other care should the patient receive? • How can we ensure that all patients get the best management?
Management of MDRTB DON’T
Estonia • Very high rates of MDRTB • Manageable annual numbers (75-100) • Small country • Single controller • Several treatment supervisors • Monthly progress meetings
England • Low rate • Manageable annual number (75-100) • Central sensitivity testing • Undesignated experts • No co-ordination of therapy • No central assessment • No outcome data • Need for co-ordination at National level
MDRTB service:Mission statement • To provide advice from an expert group to suggest optimum treatment. • To collect data on outcomes to build up a knowledge base to inform. • Participation to be voluntary
National MDR-TB Service • Agreement of relevant professional bodies • e virtual committee of experts • Give advice re: management • Patient data and progress • Follow up advice and management • Voluntary • Outcomes: bacteriological and clinical. • MDRTBservice@lhch.nhs.uk
Proposal for the management of drug resistant tuberculosis • All MDRTB specimens identified by reference lab. • Clinician managing patient informed by lab director • Clinician informed about MDRTB service • Clinician invited to contact MDRTBS re management • Asked to complete data entry form by MDRTBS • Details entered onto blog by MDRTBS • E committee informed of new case on Secure Blog. • Advice entered onto blog and emailed to managing clinician • Three-monthly clinical updates from clinician to co-ordinator. Regular meetings convened by lead clinician
Composition of virtual e-committee • Microbiologists/Lab directors 5 • Chest Physicians 13 • ID Physicians 5 • HIV physicians 1 • Paediatricians 5 • Public Health Physicians 3 • Respiratory Pharmacist 1 • TB Specialist nurse 1 • Surgeon 1 • Total 35 • Patient (1)
E mail message • A reminder of how to log on to the new MDRTB secure web based discussion forum. • (URL and log on details below, upper case essential):- • http://mdrtbservice.typepad.com/
Activity from 1/1/08 to 31/12/09 • Cases discussed (72) • (55MDR, 4XDR 13 MDR not confirmed) • Comments received 300 • Most comments (15), fewest (2) • Five most active repliers all Chest Physicians (75% of comments) • ID repliers a/c for 12% of comments
Activity from 1/1/08Questions asked • Treatment recommended • Problems with compliance • Problems with infection control • Problems with adverse reactions • Preventive therapy for contacts
Problems in implementation • Many opinions • Delay in opinions • Confused managing clinician • “Secret” managing of patients • Failure/inaccurate completion data entry forms • Confidentiality
Problems in management of patients • Achieving a consensus • drugs, monitoring, adverse events. • No designated MDRTB centres. • Role of surgery not clear. • Voluntary–need to add to guidelines?
“Political“ problems • Different specialist bodies • Chest Physicians • ID Physicians • Paediatricians • Microbiologists • Public health doctors • Specialist TB nurses
Ethical problems • Patient Confidentiality • Ethical permission: Research or Audit? • Physician liability. • Who pays? • Government: central or local? • Private.
Conclusions • Potential for best advice to be given • Follow up advice available • Outcomes recorded • Advice modified as outcomes observed • Collective wisdom • A common sense approach • Adaptable to other diseases
MDRTB the current problem (and solution) in the UK. Professor Peter Davies, Liverpool
Problems in implementation • All MDRTB specimens identified by reference lab. • Clinician managing patient informed. • Clinician informed about MDRTB service • Clinician invited to contact MDRTBS re management • Asked to complete data entry form • Three-monthly clinical updates from clinician to co-ordinator • Regular monitoring of bacteriological results • Regular input from MDRTBS. • Regular meetings convened by lead clinician
March 02, 2010 • MDRTB 77 • I would appreciate your advice on the management of a Chinese student, dob 7.7.83. • She has been in the UK for the past 18 months, studying for a PhD. She comes from Beijing, and when there about 5 years ago had an episode of haemoptysis. She had few other symptoms. Apparently CXR and CT scan showed some abnormality on the left upper lobe. I understand that no organisms were cultured. • She had had BCG as a child and gave no known TB contact history. Her University degree did involve her going in and out of the local hospital as she did a Radiology project. However there was very minimal contact with patients as she was not a medical student. • Her physicians in Beijing elected to give her a 9 month daily course of rifapentine, isoniazid and ethambutol. She reports 100% adherence and tolerated the treatment well. She had no further haemoptysis, and with minimal symptoms at onset did not feel any different on treatment. At the end of her course she had the impression from her physicians that they were not sure if she had bronchiectasis or had had TB. • About 2 years ago, still in Beijing, she recalls taking a week long course of ofloxacin for a gastrointestinal upset. Otherwise her only antibiotic exposure has been amoxicillin for sore throats. She has otherwise been fit and well and has no psychiatric history. • After arriving in the UK, last February she had another haemoptysis. She was referred to the local Respiratory Clinic . (Sequential imaging is shown below). She is HIV negative. Three sputa were smear negative, but all three grew M.abscessus (sensitive to clarithromycin and co-trimoxazole, but resistant to amikacin, cefoxitin, tigecycline, tobramycin and linezolid). • It was elected to give her treatment, but she went back to China over the summer period. On her return in the autumn she commenced treatment with clarithromycin, co-trimoxazole and amikacin (for 2 months) at the beginning of October. Clinic letters record that she had a mild cough and malaise, but she herself denies much in the way of symptoms. Subjectively she tolerated her treatment and with hardly any symptoms to begin with could not report any symptomatic improvement.
As discussed by phone regime should beCapreomycin,Pzi,Ethamb,Prothion,Cyclo,and probably PAS.One day we may know wherther PAS or linezolid is better.Also consider surgery early.Dont forget to check Vit D status • Posted by: Peter Davies | March 10, 2010 at 01:08 PM