Enterobacteriaceae
Medical Microbiology. Enterobacteriaceae. BIOL 533 Lecture 12. Enterobacteriaceae. Diversity of species Ecology Found worldwide in soil, water, vegetation, and microbial flora of animals and humans Some are always associated with disease e.g., Shigella, Salmonella, Yersinia pestis

Enterobacteriaceae
E N D
Presentation Transcript
Medical Microbiology Enterobacteriaceae BIOL 533 Lecture 12
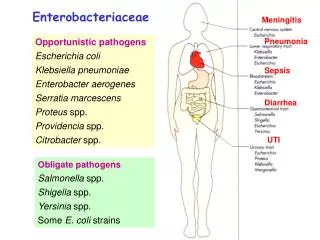
Enterobacteriaceae • Diversity of species • Ecology • Found worldwide in soil, water, vegetation, and microbial flora of animals and humans • Some are always associated with disease • e.g., Shigella, Salmonella, Yersinia pestis • Some are normal flora that can become opportunistic pathogens • e.g., E. coli, K. pneumoniae, P. mirabilis
Enterobacteriaceae • Epidemiology • Animal reservoir: most Salmonella infections • Human carrier: Salmonella typhi, Shigella • Endogenous spread in a susceptible patient • Can involve all body sites • 5% hospitalized patients develop nosocomial infections, primarily caused by Enterobacteriaceae such as Escherichia • Sites of infection
Microbial Physiology and Structure • Cell morphology • Moderate-sized Gram— rods • Non-spore-forming • Motile (with peritrichous flagella) or non-motile • Physiology • All are facultative anaerobes • Simple nutritional requirements: • Ferment glucose • Reduce nitrates to nitrites
Distinguishing Characteristics • Oxidase¯: • Distinguishes among other fermentative and non-fermentative Gram— bacilli • Lactose fermentation (red colonies on MacConkey agar) • Separate Escherichia, Klebsiella, Enterobacter from other lactose— Enterobacteriaceae
Distinguishing Characteristics • Resistance to bile salts • Separate Shigella and Salmonella from normal flora in this group • Eosin Methylene Blue (EMB) • Lactose, eosinY, methylene blue; Lac+; grow with green sheen
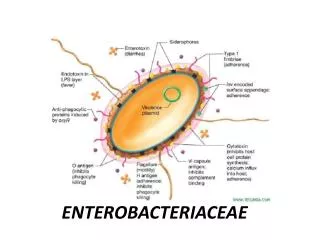
Virulence Factors • Antigens • Somatic “O” LPS • Major cell wall Ag; heat stable • Specific “O” antigens associated with each genus; however, cross reactions are common • Salmonella and Citrobacter • Escherichia and Shigella
Virulence Factors • Capsular K • Either protein or polysaccharide • Heat-labile • May interfere with detection of “O” • Removed by boiling organisms • Capsular antigen of Salmonella typhi referred to as Vi antigen
Virulence Factors • Capsular K, continued • Shared by different genera both inside and outside of family • Cross reactions • E. coli K1 with N. meningitidis and Haemophilus meningitidis • K. pneumoniae with S. pneunomiae • Organisms with specific antigens have been associated with increased virulence (e.g., E. coli K1 with neonatal meningitis)
Virulence Factors • Flagella H • Heat-labile proteins • Can be absent or undergo antigenic variation (present in two phases) • Specific H antigens assocated with disease
Virulence Factors • General role in pathogenesis of “O,” “K,” and “H” antigens • Specific antigens associated with meningitis, gastroenteritis, and urinary tract infections • Role that Ag’s play in these diseases is not clear • Some capsular Ag are poor immunogens • Protect against antibody-mediated phagocytosis • Flagellar Ag probably play a role in adherence
Virulence Factors • Pili • Attachment to host cells
Pathogenesis of Escherichia • E. coli present in gastrointestinal tract in normal flora • Bacterial sepsis (multiplication in blood) • Primary focus-infection of urinary tract or spread from gastrointestinal tract • Death can occur in immunocompromised patients and infections resulting from intestinal perforation
Pathogenesis of Escherichia • Neonatal meningitis • E. coli and group B streptococci most common • 75% E. coli possess Capsular K1 antigen • Colonization of infants with E. coli at delivery is common; disease is not
Pathogenesis of Escherichia • Urinary tract infections (80% community and most nosocomial) • Originate from gastrointestinal tract • Important virulence factors • Resistance to serum-killing • Production of hemolysins • Pili-mediated binding (not demonstrated in vivo) • Production of slime layer that participates in cell adhesion
Pathogenesis of Escherichia • Gastroenteritis (countries with poor hygiene) • Enterotoxigenic (ETEC) • Mediated by heat-labile (like cholera) and heat-stable exotoxins (activates guanylate cyclase and stimulates secretion of fluid) • Both are coded from plasmid-borne genes • World-wide:both adults and children • Incubation 1-2 days; persists 3-4 days • Mild symptoms, including cramps, nausea, vomiting, watery diahrrea
Pathogenesis of Escherichia • Gastroenteritis, continued • Enteroinvasive (EIEC) • Invade and destroy colonic epithelium • Fever and cramps with blood and leukocytes in stool • Uncommon; often food-borne • Enteropathogenic (EPEC; childhood diarrhea) • Organism adheres to enterocyte plasma membrane and causes destruction of microvilli producing watery diarrhea • Adhesiveness mediated by plasmid-encoded pili
Pathogenesis of Escherichia • Gastroenteritis, continued • Enteropathogenic (continued) • Infants< 1 year affected • Enterohemorrhagic (EHEC; hemorrhagic colitis) • Produces cytotoxin (verotoxin) • Severe abdominal pain, bloody diarrhea, little or no fever • Warm months of year; affects children < 5 years
Pathogenesis of Escherichia • Gastroenteritis, continued • Enteroaggregative (EaggEC; watery diarrhea) • Infants < 6 months • AIDS patients
Pathogenesis of Different Toxins • Cholera and ETEC • Colonize mucosal surface by toxin coregulated pilus (cholera; TcpA) or colonization factor Ag (Cfa; E. coli) • Ctx or LT binds to receptor and taken up by vesicles; transported from basolateral membrane to AC complex
Pathogenesis of Different Toxins • Cholera and ETEC (continued) • ADP-ribosylation yields cAMP (cholera-like) • ETEC (heat stable; ST) binds to membrane-bound guanylate cyclase complex that produces cGMP • Both cAMP and c-GMP reduce Na+ absorption in vilus cells • Increase CI— secretion in crypt cells; yields watery diarrhea
Pathogenesis of Different Toxins • EPEC • Attaches to small bowel by bundle forming pilus (BfpA) • Binding yields signal transduction events • Phosphorylation of major epithelial protein Hp-90 • Activation phospholipase C • Increase inositol triPO4 (IP3) and Ca • Damage to microvilli
Pathogenesis of Different Toxins • EPEC (continued) • Intimin mediates intimite association • 39 kDa protein causes polymerization of actin and other cytoskeletal proteins and rearrangement of cytoskeletal structure • Form characteristic EPEC pedestal (attaching effacing lesion) with intimately attached organism; not known how host gets diarrhea)
Pathogenesis of Different Toxins • Interestingly, E. coli 0:157H:7 has pedestal and Shiga toxin (char. Shigella)
Pathogenesis of Salmonella • Source of most infections • Ingestion of contaminated water, food • Poultry, eggs, and dairy products • Salmonella typhi spread by food or water; contaminated by food-handlers • Need to ingest large number of organisms (106-8) • By fecal-oral contact in children
Pathogenesis of Salmonella • Gastroenteritis (most common) • Symptoms 6-48 hours after ingestion • Nausea, vomiting, non-bloody diarrhea • Elevated temperature, abdominal cramps, muscle cramps, headache • Symptoms persist for 2 days to a week before abating • Antibiotics are normally not employed because carrier state can develop
Pathogenesis of Salmonella • Gastroenteritis (continued) • More acid-sensitive than Shigella • Infect patients with decreased stomach acid • Large inoculum needed • Decreased by 10-100X in the presence of bicarbonate
Pathogenesis of Salmonella • Septicemia (pediatric and geriatric patients) • 10% patients can get: • osteomyelitis, • endocarditis, or • arthritis
Pathogenesis of Salmonella • Enteric fever (S. typhi, typhoid; S. paratyphi, paratyphoid) • Paratyphoid is milder • Symptoms after 10-14 day incubation period • Gradually increasing remittant fever • Headache, muscle aches, malaise, and decreased appetite; gastrointestinal symptoms occur • Symptoms persist for a few days
Pathogenesis of Salmonella • Enteric fever (continued) • Carriers (“Typhoid Mary”) • 1-5% of patients will carry after a year • Gall bladder-primary source
Mechanism of Pathogenesis • Sense acid environment produces ~40 proteins with importance to pathogenesis • Organisims escape killing in: small bowel, and distal illeum of colon • Penetrate mucosal barrier; not clear whether involves: • M cells -OR- • apical membrane of gut epithelial cells -OR- • Tight junction between cells
Mechanism of Pathogenesis • Sense acid environment (continued) • Contact of organism’s cells in culture producing ruffling of plasma membrane (cytoskeletal rearrangements) lead to uptake into phagocytic vesicles • Interaction with epithelial cells activates inflammatory response yielding damage to intestinal mucosa
Mechanism of Pathogenesis • Interaction with epithelial cells (continued) • Assembly non-pili appendages (15 minutes) • S. typhimurium • 14 genes of inv operon • In 30 minutes, ruffles appear • Bacterial appendages disappear • Assembly mutants: both assembly and disassembly • inv A E assemble; never disassemble • inv C G never assemble
Mechanism of Pathogenesis • Biochemical events activated during invasion • Activation: mitogen activated • Protein kinase (MAP kinase) • Linked to surface receptor • Binding produces activation • Phospholipase A2 (PLA2) • Release arachidonic acid • Produce prostaglandin leukotrienes • Increase in intracellular Ca+2
Mechanism of Pathogenesis • Biochemical events (continued) • All these produce ruffling, but also alter electrolyte transport leading to diarrhea • Bacteria remain in vesicles for hours • Resistant to lysosomal contents and antibacterial peptides made by intestinal epithelial cells (cryptins) • Move from vesicles to basement membrane leading to lamina propria
Mechanism of Diarrhea • Exact mechanism of diarrhea unknown • Invasion produces IL8 that leads to local leukocyte attraction • Ability to invade and produce inflammation necessary, but not sufficient to produce diarrhea; found by experiments in animals • Other signal necessary • Some have cholera toxin-like molecule
Pathogenesis of S. typhi • Typhoid Fever • Survive in macrophage; studied in mice • Causes typhoid-like illness in mice; diarrhea in humans
Pathogenesis of S. typhi • Virulence regulated signal transduction (PhoP/PhoQ) • Mutations • Decreased survival in macrophage • Increased sensitivity to acid pH • Sensitivity to mammalian antimicrobial peptides • Attenuation of virulence
Pathogenesis of Salmonella • Invasive non-typhoidal strains • Virulence plasmid • 8 kb conserved Salmonella plasmid virulence genes (spv) • Turned on: • when enter eukaryotic cells • resistance to complement
Properties of Shigella • Species • Shigella sonnei (industrial countries) • Shigella flexneri (underdeveloped countries) • Pediatric disease (1-4 years) • Associated day-care centers, nursuries, and custodial institutions • Spread by fecal-oral route (hands) • 200 bacilli can establish disease
Properties of Shigella • Clinical syndromes (1-3 days after ingestion) • Abdominal cramps • Diarrhea • Fever • Bloody stools
Properties of Shigella • Pathogenesis • Colonize small intestine and multiply during first 12 hours • Initial sign of infection—profuse watery diarrhea without histological evidence of mucosal invasion • Mediated by enterotoxin • Invasion of colonic epithelium results in lower abdominal cramps, difficulty defecating, abundant pus and blood in stool • Bacteremia is uncommon
Antibiotic Therapy of Shigella • Antibiotic treatment is recommended to reduce spread to other contacts • Fluoroquinolines-adults • Under 17-damage to cartilage and joints • Determined by animal studies • FDA does not allow use in children • New -lactam cephalosporin in use
Pathogenesis of Shigella • Survival in stomach • Sense acid environment • Sigma factor RNA polymerase (formed in stationary phase)
Pathogenesis of Shigella • Survival in stomach (continued) • Controls group of genes concerned with acid resistance; acid resistance increased • Invasion-ability less • When reach small intestine, invasion ability returns and acid resistance repressed • Acid resistance enhanced by anaerobic conditions found in large intestine • Likely when excreted: acid-resistance is expressed; ready for next host
Large Intestine Invasion • Bacterial multiplication occurs inside intestinal epithelial cell • Invasion and survival • multiple genes both on chromosome and plasmid (large virulence)
Large Intestine Invasion • Invasion steps • Get close to mucosal surface (unknown mechanism); no flagella; non-motile; cells can’t be invaded on luminal surface, but can be on basal • First enter M cells (Ag sampling cells) • Depends on plasmid coded outer membrane proteins • Invasion plasmid Ag; IpaB C D
Large Intestine Invasion • Invasion steps (continued) • Released into lamina propria (intercellular space) • ingested by macrophage • They release IL1 that produces inflammatory response; increase subsequent invasion close to basal surface • Entry of Shigella into mucosal epithelial cells; rearrangement of actin cytoskeletal elements
Large Intestine Invasion • Invasion steps (continued) • Go from phagosome into cytoplasm and mutiplies • How do they infect other cells? As they multiply, they make protein IcsA that causes intracellular spread of 1 pole of rod; ATPase causes polymerization of actin (host)
Large Intestine Invasion • Deposition of actin propels bacteria forward • Fingerlike projection pokes adjacent cell • Surrounded by a combination of old and new membrane; produces lysis and entry of organism into cytoplasm of new cell