Download
1 / 11
120 likes | 309 Views
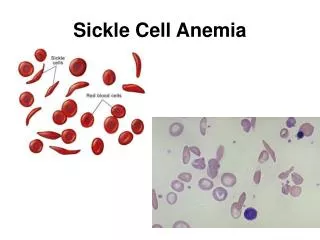
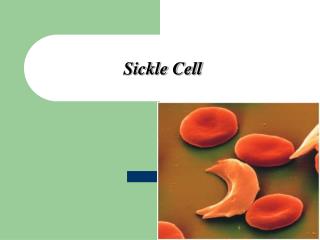
Sickle Cell Pain Crisis and Fever Management. PEM 102. Sickle Cell. All varieties at risk for pain crisis including: Homozygous Hgb SS Heterozygous Hgb SC Sickle Beta thalasemia, variable complications 60% will have vaso-occlusive crisis by 2yo

E N D
Sickle Cell • All varieties at risk for pain crisis including: • Homozygous Hgb SS • Heterozygous Hgb SC • Sickle Beta thalasemia, variable complications • 60% will have vaso-occlusive crisis by 2yo • Dactylitis and acute pain are most common presenting symptom
Acute Painful Crisis • Precipitated by illness, dehydration, stress, menses • Most common locations include back, chest, abdomen, and extremities • Duration typically 2-7 days • Mechanism under debate • Direct occlusion of capillaries and recruitment of inflammatory mediators IL-6, IL-8, substance P
ECH Pain Management • Rapid triage on arrival – red triage • History • Location, duration, and severity scale • Consider other etiologies: appy, cholecystitis, trauma • Analgesic use at home, timing of last dose • What works in the past
Physical Exam & Labs • See fever pathway if > 38.3 • Oxygen for hypoxia less than baseline • Lungs, spleen, bones/joints, GU, neuro exam • Labs: • CBCD, Retic (compare to baseline), +/- T&S • UA if abd/flank pain and symptoms • CXR if fever, chest pain, tachypnea • Consider RUQ U/S, LFT’s, pelvic exam if needed
Treatment • Based on severity of pain, recent home analgesics, and prior experience of patient • Often receive Lortab at triage • Consider NSAIDs and opiates • Toradol 0.5mg/kg (max 30mg) IV q6 OR Motrin • Morphine 0.1-0.15mg/kg q30min • Dilaudid 0.015-0.02mg/kg • Nalbuphine (Nubain) 0.2-0.3mg/kg q3h • Avoid Demerol (inc risk sz with repeated doses) • IVF: 10cc/kg NS over 1hr then D5 ¼ NS at MIVF
Management and Admission? • Look at previous visits to see what works • If frequent visits or concerns about drug-seeking noted on previous visits call consultant early to determine plan • After treatment, discuss options with family • If resolution with opioid x 1 consider oral analgesic and observation in the ER for rebound pain • If more than one or two doses required consider admission • Discuss case and plan with on-call consultant
Sickle Cell and Fever • Splenic dysfunction from Hgb S leads to impaired splenic filtration → auto-infarction by 2-4yo • Impaired IgG and IgM responses and complement dysfunction also play a role • Increased susceptibility to encapsulated microorganisms • especially Streptococcus pneumo and H. influenzae • PCN at 125mg BID to 3yo then 250mg Bid at 5yo • Pneumococcal sepsis can occur on PCN, usually associated with sub-optimal compliance • Safe to stop PCN ppx at 5yo if 2 doses of 23-valent vaccine and no significant history of sepsis
Sickle Cell and Fever (>38.3) • Rapid triage on arrival • Compliance with PCN, history of SBI, ACS • Examine for evidence of systemic of localized infection • Labs based on protocol: • CBCD, Retic, Blood cx, consider CRP • Consider UA and Ucx without other source • CSF based on clinical examination • Type & Cross for pallor, AMS, enlarged spleen – leukocyte depleted sickle negative pRBC (match for minor Ag if possible)
Management • Prompt Ceftriaxone 50-75mg/kg (2g max) IV • Give IM if access delayed • If known allergy consider meropenum • Severe illness with AMS, hypotension add vancomycin • IV Abx immediately after blood cx and before procedures • Presence of foci (ASOM, Strep throat) does not alter urgency for Abx • Add atypical coverage if CXR + and > 2yo
Management • NS bolus 10-20cc/kg for dehydration, hypotension, MIVF for well hydrated pts • CXR if: • cough, resp symptoms, tachypnea, chest or abd pain, abnl exam, Pox less than baseline • Sickle cell consult: • Likely admit if < 1yo, previous SBI, Temp >40, WBC >30 or < 5, plt < 100, CXR +, co-existing acute pain, or social concerns • Outpt management: minimum of phone f/u to repeat exam and Ceftriaxone at 24hrs (with or without repeat CBC)