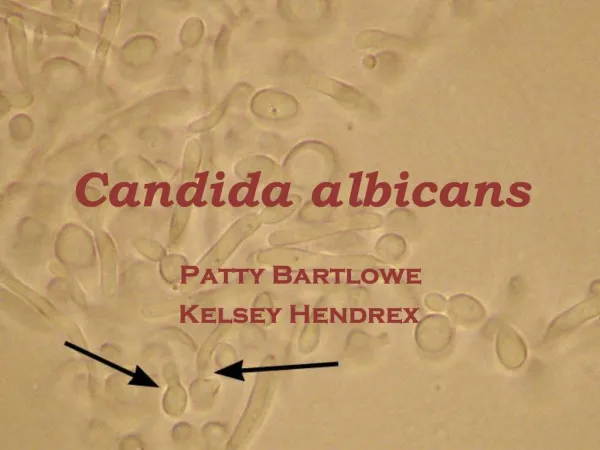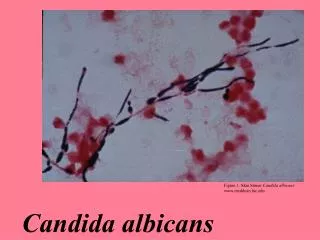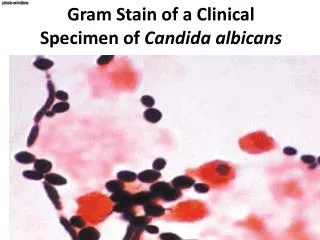

Candida albicans
E N D
Presentation Transcript
Miscellaneous bacteria:chlamydiae, neisseriae & spirochetes Dr. Taseen S. Desin (Ph.D.)
Objectives • Chlamydiae • Discuss the classification of Chlamydia • Differentiate between the clinical presentation of Chlamydia trachomatis, Chlamydia psittaciand Chlamydia pneumoniae • Neisseria gonorrhea • Discuss the clinical features and epidemiology of these sexually transmitted diseases • Spirochetes (Syphilis): Treponemapallidum • Discuss the classification of Spirochetes • Discuss the primary, secondary and tertiary stages of syphilis
Chlamydia species • Gram negative • Obligate intracellular parasite • Small, round-to-ovoid organisms • Vary in size during different stages of their life cycle • They synthesize their own proteins • Sensitive to inhibitors of protein synthesis [tetracyclines& macrolides.] • Do not grow on laboratory media • Require living cells for growth (embryonatedeggs or in tissue culture cells) • Genitourinary tract and eye infections • Chlamydia trachomatis • Respiratory tract infections • Chlamydia psittaci • Chlamydia pneumoniae
Elementary body Chlamydia species - Pathogenesis Reticulate body Unique Life cycle Infectious form Elementary body: initiates an infection & once phagoyctosed prevents fusion of the phagosome and lysosome, protecing itself Reproductive form Reticulate body: multiplies by binary fission to increase in number Elementary body
Chlamydia Trachomatis –Clinical significance (1) • C. Trachomatis causes a range of Genitourinary tract and Eye Infections • Nongonococcal urethritis (NGU) • > 4 million cases/year in the U.S. (most common STD) • Males: urethra is affected • Females: cervicitis and/or urethritis • Infections can be asymptomatic • Infections may spread: • Men: Epididymis • Women: Fallopian tubes & adjacent tissues (pelvic inflammatory disease) • Chlamydial NGU is similar to infections caused by Neisseria gonorrhea except: • Longer incubation period (2-3 weeks) • Discharge is more mucoid (less pus cells) • Treatment: NGU and Neisseria gonorrhea
C. Trachomatis – Clinical Significance • Lymphogranuloma venereum (LGV) • Invasive sexually transmitted disease • Common in Asia, Africa and South America • Papules on external genitalia, followed by painful swelling of inguinal & perirectal lymph nodes • Trachoma • Chronic keratoconjunctivitisoften leads to blindness • Transmitted by personal contact • Eye to eye via droplets • Contaminated surfaces touched by hands • Persistent or repeated infection leads to blindness • Neonatal conjunctivitis • Affects >50% of infants born to women infected with C. trachomatis • Symptom: inclusion conjunctivitis and may cause pneumonia • Requires antibiotic treatment. • If untreated, can cause permanent eye damage • Adults infected with C. trachomatis may also develop conjunctivitis Adult inclusion conjunctivitis
C. trachomatis – Identification & Treatment Flourescent antibody staining Identification Samples from Urethra & cervix (GU) and conjunctivae (ocular) Flourescent antibody staining (immunoflourescence) PCR – polymerase chain reaction to amplify DNA Culture: does not grow on media (tissue culture – human cell lines) Treatment Erythromycin, Azithromycin, Doxycyline C. trachomatis grown in tissue culture
Chlamydia psittaci& Chlamydia pneumoniae • C. psittaci • Causes: Psittacosis or Ornithosis • Zoonotic disease transmitted to humans from the inhalation of dust contaminated with respiratory secretions or feces of infected birds • Affects the lower respiratory tract • Flu-like symptoms – enlargement of liver and spleen • Severity: asymptomatic to fatal (rare) • Workers who deal with birds (high risk) • Diagnosis: antibody titers by immunoflourescence • Treatment: Doxycycline or Erythromycin • C. pneumoniae • Causes Pharyngitis, followed by Laryngitis, bronchitis or pneumonia • Significant cause of community-acquired respiratory infection • Treatment: Doxycycline or Erythromycin
Neisseria gonorrhoeae • Gram negative, aerobic cocci (diplococci) • Transmission • Sexual contact • During the passage of a baby through an infected birth canal
N. gonorrhoeae - Pathogenesis • Structure • Pili • Hairlike surface appendages that enhance attachment to host cells • Resistance to phagoyctosis • Lipooligosaccharide (LOS) • Shorter, more branched O-antigenic side chains than LPS • Opacity proteins • Mediate attachment • Pathogenesis • Attach & colonize epithelial cells of the urethra, rectum, cervix, pharynx or conjunctiva • IgA protease – destroys IgA • Colonizes mucous membranes of the GU and/or rectum • Localized infections are characterized by pus • May lead to tissue invasion and chronic inflammation • Females are often asymptomatic • Act as reservoirs for maintaining and transmitting gonococcal infections • Often more than one sexually transmitted disease is acquired at the same time requiring treatment for more than 1 pathogen
N. gonorrhoeae– Clinical Significance • Genitourinary tract infections • Males: yellow, purulent urethral discharge & painful urination • Females: infection in the endocervix which extends to the female genital tract (greenish-yellow discharge) • Can progress to the uterus, causing salpingitis (inflammation of the fallopian tubes infertility ~ 20%), pelvic inflammatory disease & fibrosis) • Rectal infections • Prevalent in male homosexuals • Symptoms: constipation, painful defecation & purulent discharge • Pharyngitis • Oral-genital contact purulent pharyngeal exudate • Opthalmianeonatorium • Infection of conjunctival sac acquired during birth • May lead to blindness if untreated • Disseminated infection results from gonococcalbacteremia. • Fever, painful arthritis, small pustules on the skin • More common in women • Patients treated should also receive treatment for Chlamydia
N. Gonorrhoeae– Identification & Treatment • Identification • Male: neutrophils containing gram negative diplococci in urethral discharge allows for treatment • Females: a positive culture is required to confirm infection in urethral discharge • Disseminated gonococcal infection culture confirmation required • Culture of skin lesions, joint fluid or blood. Thayer – Martin chocolate agar • Treatment • Cephalosporins • Partners in relationships should be treated • No effective vaccine available • No natural immunity • Prevention: safe sexual practices (especially with multiple partners)
Treponemapallidum • Sexually transmitted infection caused by the spirochete Treponemapallidum(T. pallidum) • Gram negative bacilli that have a characterisitic corkscrew or helical shape • Causes Syphilis • First sign: Small lesion – chancre • 3 progressive stages of disease • Can last 30 years or more • May lead to syphilitic dementia or cardiovascular damage Spirochete morphology
T. Pallidum Pathogenesis • Transmission: • Sexual contact or transplacentally (congenital syphilis) • Entry: break in the skin or penetration of mucous membranes (genitalia) • T. pallidumcannot survive outside of the host for long • Syphilis occurs in 3 stages • Primary Syphilis • Secondary Syphilis • Tertiary Syphilis
T. Pallidum– Clinical significance (1) Primary Syphilis Hard, painless genital or oral chancre at site of inoculation 3 weeks between infection and appearance of chancre Lesions heal but organism continues to spread via lymph & blood Asymptomatic period for up to 24 weeks Secondary Syphilis Rashes and papules on almost any part of the body (the palms of the hands and soles of the feet, in mouth and armpits) Primary & secondary lesions extremely infectious Other organs may also be involved – liver, brain, kidneys • Tertiary Stage (40% of individuals) • After healing of secondary lesions, the disease enters a latent period, this stage can last many years • Degeneration of the nervous system & lesions (granulomatous lesions = gummas) in deep organs like the heart, liver, skin
T. pallidum– Clinical significance (2) • Congenital syphilis • T. pallidumis transmitted through the placenta to a fetus after the first 10-15 weeks of pregnancy • Death & spontaneous abortion of the fetus are possible or still birth • Infected infants who live develop a condition similar to secondary syphilis including a variety of CNS & structural abnormalities • Treatment • Treatment of the mother with appropriate antibiotics prevents this disease
T. pallidum– Identification & Treatment • Identification • Cannot be easily cultured • Immunoflourescent staining and dark-field microscopy • Antibody titers – ELISA • Treatment • Penicillin • No vaccine available • Safe sexual practices • **Multiple Diseases may need to be treated** Dark-field microscopy [T. pallidum] Immunofluorescence microscopy