Download
1 / 6
60 likes | 91 Views
Anemia and iron deficiency are the most frequent nutritional problems on the worldwide scale. Haemoglobin, the<br>iron containing metalloprotein in the red blood cells, transports oxygen from the lungs to the rest of the body, where<br>it releases its load of the oxygen. Depletion of iron concentration leads to inhibition of haemoglobin synthesis<br>causing iron deficiency anemia. Mainly women are at the risk of developing iron deficiency. Taking this into<br>consideration estimation of iron concentration and haemoglobin level from blood samples of 96 working women<br>volunteers from various age groups is carried out. Haemoglobin level estimated by using CMG method and iron<br>concentration determined by atomic absorption spectroscopy technique. In the samples iron concentration and<br>haemoglobin level are found to be in the range of 119 to 970 ppm and 8.8 to 18.7 g/dL respectively. 44 cases<br>showed haemoglobin level lower than the normal range indicating anemic condition. On the other hand iron<br>concentration and haemoglobin level in 10 cases was found to be in the normal range. 37 cases showed iron<br>concentration lower than normal range though haemoglobin level was within normal reference range. Iron concentration and haemoglobin level in remaining 5 cases was found to be more than normal range.

E N D
Available online www.jocpr.com Journal of Chemical and Pharmaceutical Research, 2012, 4(4):2300-2305 ISSN : 0975-7384 CODEN(USA) : JCPRC5 Research Article Assessment of iron and haemoglobin status in working women of various age groups 1,3*N. S. Rajurkar, 2S. F. Patil and 3N. H. Zatakia 1Department of Chemistry, University of Pune, Pune 2Bharati Vidyapeeth, Pune 3Department of Environmental Sciences, University of Pune, Pune _________________________________________________________________________________________ ABSTRACT Anemia and iron deficiency are the most frequent nutritional problems on the worldwide scale. Haemoglobin, the iron containing metalloprotein in the red blood cells, transports oxygen from the lungs to the rest of the body, where it releases its load of the oxygen. Depletion of iron concentration leads to inhibition of haemoglobin synthesis causing iron deficiency anemia. Mainly women are at the risk of developing iron deficiency. Taking this into consideration estimation of iron concentration and haemoglobin level from blood samples of 96 working women volunteers from various age groups is carried out. Haemoglobin level estimated by using CMG method and iron concentration determined by atomic absorption spectroscopy technique. In the samples iron concentration and haemoglobin level are found to be in the range of 119 to 970 ppm and 8.8 to 18.7 g/dL respectively. 44 cases showed haemoglobin level lower than the normal range indicating anemic condition. On the other hand iron concentration and haemoglobin level in 10 cases was found to be in the normal range. 37 cases showed iron concentration lower than normal range though haemoglobin level was within normal reference range. Iron concentration and haemoglobin level in remaining 5 cases was found to be more than normal range. Key words: IDA, Iron estimation, Haemoglobin, Women, Spectrophotometer. _________________________________________________________________________________________ INTRODUCTION Anemia is a result of wide variety of causes that can be isolated, but more often coexists. The most significant contributor of anemia is iron deficiency and it is generally assumed that 50 % of the cases are due to iron deficiency [1] and is one of the common nutritional deficiencies in the world affecting the absorption and metabolism of other antioxidant minerals including copper and selenium [2]. According to the world health report 2002 Reducing risk and promoting healthy life, nutritional iron deficiency was identified as one of the 10 leading risk factors for disease, disability and death in the world [3]. Thus global public health problem affects both developing and developed countries with major consequences for human health as well as social and economic development. Though it occurs at all stages of life cycle, it is found to be more prevalent in women of all ages [4]. Iron is critical part of many enzymes and is a vital component of haemoglobin in red blood cells. Haemoglobin is a complex molecule, composed of protein (globulin) and heme group, which contains iron atom and is responsible for the binding of oxygen and transport of O2 throughout the body. Each red blood cell contains 200-300 haemoglobin molecules which are produced in bone marrow in the presence of iron only. The main risk factors for iron deficiency anemia (IDA) include a low intake of iron, poor absorption of iron from diets which are high in phytates or phenolic 2300
N. S. Rajurkar et al ______________________________________________________________________________ J. Chem. Pharm. Res., 2012, 4(4):2300-2305 compounds. Iron deficiency adversely affects work performance, cognitive functioning, immunity and thermoregulation [5-9]. Hence it is thought of interest to estimate iron concentration and haemoglobin level in the working women of various age groups. EXPERIMENTAL SECTION Subjects: A cross sectional study was carried out for assessment of iron concentration and haemoglobin level in working women from Pune city, Maharashtra, India. For this study 95 working women in age group of 20 - 60 yrs participated voluntarily. Sampling: 5 ml blood from subjects were drawn by vein puncture under contamination controlled conditions with disposable syringe and transferred in vacuettes which contain K3EDTA as an anticoagulant. These samples were stored in the freezer at -20 o C till the analysis. Haemoglobin determination by Cyanmethemoglobin method: In this study haemoglobin content is determined by cyanmethemoglobin method within 24 hrs after obtaining the blood samples. For this purpose the blood sample is mixed with Drabkin's solution, a solution that contains ferricyanide and cyanide. The ferricyanide oxidizes the iron in the haemoglobin, after that haemoglobin changes to methemoglobin. Methemoglobin then unites with the cyanide to form cyanmethemoglobin which is coloured. Its absorbance is measured on a spectrophotometer at 540 nm. This absorbance is related to the concentration of haemoglobin in the blood which is expressed as g / dL. Estimation of iron in blood sample by Atomic absorption spectrometer: The blood sample is mixed with digestion acid (HNO3 + H2SO4 + HCIO4 in 3:1:1 proportion) in 1:1 ratio and digestion is carried out in round bottom flask with attached condensers by continuous heating at constant temperature of 110 oC for about 3 hrs. Towards completion of digestion, clear solution is obtained. This solution is diluted with Milli-Q water for further analysis. The absorbance of the sample was measured on Perkin-Elmer 3100 atomic absorbance spectrometer at the wavelength of 248.3 nm and 0.2 nm slit width with a lamp current of 20 mA. The absorbance values were measured by aspirating the solutions in the order of blank, standards and samples into the air acetylene flame. A minimum of three absorbance values were recorded for each solution and the mean value of the absorption signal was used for subsequent calculations. The absorption signal was evaluated by subtracting the value of blank from the signal of the sample. RESULTS AND DISCUSSION Hemoglobin concentration is the most reliable indicator of anemia at the population level and its measurement is relatively easy and inexpensive. It is frequently used as proxy indicator of anemia which can cause by the factors other than iron deficiency [10]. Hemoglobin levels of the subjects under study were estimated by cyanmethemoglobin method [11-14] and are shown in Table 1 and Figure 1. The iron content of whole blood samples of different subjects is estimated by atomic absorption spectroscopy method and results are given in Table 1 and Figure 2. All these results are an average of 3 independent measurements with relative deviation of ± 0.3 %. Table 1: Variation of iron and haemoglobin level in working women of different age groups Sr. No. Age / yrs Fe / ppm 1 30 2 21 3 22 4 27 5 23 6 21 7 23 8 20 Hb / gm dL-1 13.6 14.5 13.6 12.2 11.8 10.9 11.3 11.8 119.4 222.8 208.8 349.4 878.8 197.8 270.3 261.2 2301
N. S. Rajurkar et al ______________________________________________________________________________ J. Chem. Pharm. Res., 2012, 4(4):2300-2305 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65 66 67 68 69 70 71 72 73 74 51 48 23 22 58 53 30 42 23 23 35 21 23 21 22 37 33 29 23 22 22 22 22 23 22 27 22 25 22 22 25 27 22 56 26 23 35 39 32 58 36 23 25 22 21 39 58 23 40 22 25 21 40 23 24 22 23 24 22 23 24 23 22 23 23 23 159 364.6 474.8 164.6 223.2 474.2 957.4 408.7 194.6 216.4 206.4 484.2 226.6 783 496.8 632.2 214.8 175 239 214.4 197.4 211.8 206.2 102.6 284.6 337 165.4 416.8 485.7 292.8 142.8 212 233 348.3 305.6 265.4 358 234.6 349.8 248.6 310 389.2 422.6 487.8 132 602.8 450.4 498.6 242 358.6 123.5 105.6 244 362.2 231.4 424.4 223.8 226.4 231.4 206.8 617.4 139.8 138.26 144 203.6 526.8 12.2 12.2 10.9 9.9 9.5 11.3 10.4 12.2 15.5 13.1 16 12.2 9.9 15 16 14 11.3 12.2 14 11.3 13.1 12.2 13.1 13.1 12.7 12.7 12.2 12.7 11.8 11.8 9.9 10.9 12.2 12.2 10.4 12.7 12.2 12.2 12.2 11.8 10.4 13 9.9 11.8 11.8 13.6 10.4 9.9 9.9 8.6 12.2 12.2 9 11.8 12.7 15 12.2 12.7 14.5 11.8 9.9 11.3 9.5 13.1 10.9 12.2 2302
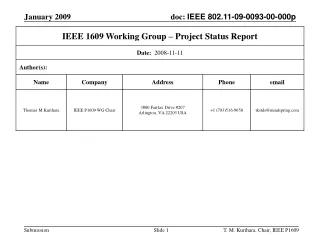
N. S. Rajurkar et al ______________________________________________________________________________ J. Chem. Pharm. Res., 2012, 4(4):2300-2305 75 76 77 78 79 80 81 82 83 84 85 86 87 88 89 90 91 92 93 94 95 32 22 22 23 48 23 60 21 23 22 47 20 21 22 22 32 21 42 21 23 23 144 399 108.8 325.6 970.7 601.4 182.6 433.6 122.2 360.4 155.2 107.4 405.8 250.2 482.4 215.8 133.4 632.8 243.4 540.8 710.2 10.4 10.4 10.9 11.3 13.1 13.6 14.5 14 12.7 11.3 13.1 11.3 9 12.2 13.6 14 13 10.9 14.5 15.5 13.6 16 norm al range of haem oglobin 14 -1 Haemoglobin / g dL 12 10 8 20 30 40 50 60 Age / y Figure 1: Hemoglobin level among working women of age group 20 to 60 years. 2303
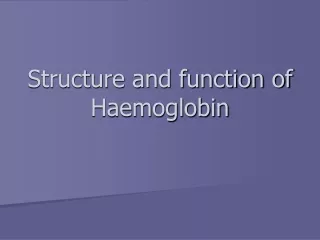
N. S. Rajurkar et al ______________________________________________________________________________ J. Chem. Pharm. Res., 2012, 4(4):2300-2305 1000 800 Fe / ppm 600 Normal Reference range of Fe 400 200 0 20 30 40 50 60 Age / y Figure 2: Iron concentration in whole blood of the working women of age group 20 to 60 years An examination of Figs. 1 and 2 shows that iron content of working women from different age groups varies between 119 to 970 ppm and haemoglobin level between 8.8 to 18.7 g/dL while the normal range of the former is 400 - 600 ppm and that of later is 12.5 to 15.5 g /dL. Further exercitation of results reveal that among the subjects studied 10 women showed normal iron and haemoglobin level, 5 are found to have more iron and haemoglobin, 29 with less iron and haemoglobin as compared with the normal reference range while 12 cases showed less haemoglobin but normal iron and 37 cases showed iron concentration lower than normal range still haemoglobin level is within normal reference range. Haemoglobin estimation in blood sample is of prime importance in medical investigations. It is advised in every admitted case and in all females undergoing antenatal check up. Hemoglobin is porphyrin iron protein compound that transfers oxygen from the lungs to the body tissues where it utilized for energy metabolism [15]. A low haemoglobin is referred to as anemia and is defined as reduction in number of or volume of circulating red blood cells (erythrocytes) or an alteration in haemoglobin. There are 400 types of anemia. The origin of anemia is classified as either nutritional or non nutritional. Anemia of nutritional origin are those that stem from deficiency of some nutrient, mainly iron, vitamin B 12 or folic acid, vitamin B2, vitamin B6, C, A, D, E and K as well as zinc, calcium, protein. Non nutritional causes are those that produce decreased development of red blood cells precursors decreased erythropoieses or an increase destruction of RBC’s [16-17]. Thus 12 subjects under study indicate that the condition of anemia is not due to iron deficiency but may be due to other reasons. 29 subjects clearly indicate iron deficiency anemia. Iron deficiency anemia is one of the common forms of anemia, which occurs when body lacks mineral iron to produce the haemoglobin it needs to make red blood cells. This is a highly prevalent in women in developing countries [18-20]. It is reported in the literature that the effects of iron deficiency on work performance, short term memory, attention span, reduced resistance to infection, reduced ability to maintain body temperature, may impact negatively on the health and well being of women, including their fatigue level [21]. 37 cases show normal haemoglobin but are deficient in iron concentration which may be proned to anemic condition in future. In case of 5 subjects both iron and haemoglobin concentrations are found to be more than normal. This condition may be due to dehydration which causes falsely high haemoglobin and iron concentration which disappears when proper fluid balance is restored. 2304
N. S. Rajurkar et al ______________________________________________________________________________ J. Chem. Pharm. Res., 2012, 4(4):2300-2305 The present study reveals that even if there is enough iron in blood, the haemoglobin can be low or vise versa as there is no direct correlation between iron concentration and haemoglobin level in blood. Thus may be due to intrinsic and extrinsic factors which affect haemoglobin metabolism causing anemia. Acknowledgement Authors are thankful to University of Pune for financial assistance. REFERENCES [1]Iron deficiency anemia: assessment, prevention and control. A guide for programme managers. Geneva, World health organization 2001, (WHO/ NHD/01.3) [2]S. Gropper, S. Kerr and J. Barksdale, Nutritional biochemistry, 2003, 14, 409-415. [3]WHO. The world health report 2002 – World health organization, 2002. [4]H. Tapiero, L.Gate, K. Tew, Biomed Pharmacother2001, 55,324-32. [5]S. Basta, D. Soekirman, D. Karyadi, N. Scrimshaw. Am J. Clin Nutr. 1979, 32, 916-925. [6]F. Oski , A. Honig, B. Helu, P. Howanitz. Pediatrics1983, 71 (6), 877-880. [7]B. Lozoff, G. Brittenham, F. Viteri, A. Wolf, J. Urrutia. J Pediatric1982, 101, 948-952. [8]E. Pollitt, P. Hathirat, N. Kotchabhakdi, L. Missell, A. Valyasevi. J Clin Nutr1989, 50 (3 Suppl), 687-96. [9]M. Andelman,B. Sered. Am J Dis Child1966, 111, 45-55. [10]Worldwide prevalence of anemia .WHO global database on anemia 1993-2005. [11]H. Qurshi. Pakistan Journal of Medical research1999, 38(4), 149-50. [12]M. Cheesbrough. Cambridge University Press 2000, 267-347. [13]Hematology Section 2. The College of American Pathologists (CAP) Laboratory Accreditation Program checklist 2000. [14]K. Ward, C. Lehman, A. Leiken . Philadelphia, WB Saunders Company 1994. [15]E. Dessparis. Erythropoiesis In: Foester J, Paraskevas F, Grear J, Rodgers G eds. Wintrobes clinical hematology. Williams Wilkins Baltimore 1999, 169-227. [16]Worldwide prevalence of anemia, WHO global database on anemia 1993-2005. [17]T. Gangadhar, P. Srikanth, and Y. Suneetha. J. Chem. Pharm. Res., 2010, 2(3), 400-410. [18]S. Redman, D. Hennrikus, J. Bowman , Sanson – Fisher R. Med J Aust1988, 148, [19]123-7. [20]W. Brown, F. Doran. Aust NZ J Public health1996, 20(2), 149- 154. [21]V. Walters. Can J Public health1992, 83, 371-4. [22]J. Amanda, J. Wendy, D. Roberts. Nutrition Research1998, 18, 489-502. 2305