Download
1 / 12

E N D
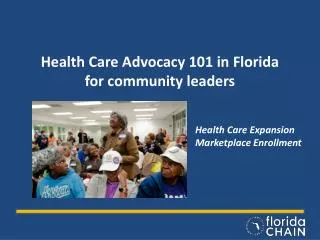
1. AMA 101 Communications in Health Care
3. Health Care Employee Role in Communication Communicates effectively, accurately and appropriately with
physicians, staff members and patients
Use proper grammar
Be professional
MA often is the first person the patient meets, you represent your physician
Positive attitude
Therapeutic communication
Clarify confusing messages
Confirm or validate patient�s perceptions
Adapt messages to patient�s level of understanding
Ask for feedback
4. Verbal & Non-Verbal Communication Verbal � exchange of messages using words or language; most common
Polite
Professional
Proper grammar
Gear conversation to patient�s educational level
Paralanguage � tone, quality, volume, pitch and range
Non-language � laughing, sighing, sobbing, grunting, etc�
Written � clear, concise, accurate
Non-Verbal � exchange of messages without using words (body language); may reflect more accurately a person�s true feelings
Kinesics � body movements, facial expressions, gestures and eye movements
Proxemics � spatial relationships or physical proximity; personal space; 3 feet
Touch � therapeutic indicates support, concern, feeling; use good judgment, read body language first
6. Interview Techniques Active listening � give full attention, try not to interrupt, observe body language or non-verbal as well as verbal, ask appropriate questions, record answers; use the following techniques:
Reflecting � repeat what patient says using open-ended questions; allows for further comments
Paraphrasing � repeat what you hear, using your own words or phrases; allows for clarification
Clarification � asking patient to give an example; helps to understand what patient is saying and gives insight on perception
Open-ended questions � best way to obtain info; allows for elaboration; use questions that start with: what, when or how, do not use why. Close-ended questions are answered by yes or no, avoid these
Summarizing � review of info for clarification or organization
Allowing silence � natural and gives time for thought formulation
7. Barriers to Communication
Clich�s � do not use, can be demeaning
Culture � be sensitive to differences in beliefs, body language can be misunderstood
Stereotyping � holding opinion of all members of a particular culture or race; discriminatory
Bias � personal opinions; treat all patients fairly, respectfully and with dignity regardless of who they are
Language � use an interpreter, do not shout, use simple English if possible, avoid slang, learn basic phrases in other languages
Hearing impairment � talk face to face, use interpreter, use written notes, use visual aids
8. Barriers cont�
Sight impairment � identify yourself, do not raise voice, describe what
you are doing each time, offer your arm, orient patient spatially, explain
sounds of machines to be used
Speech impairment � allow patients time to gather thoughts, allow time to communicate, offer note pad to write
Mental health issues � explain what to expect, keep conversation focused, do not be demanding or forceful, orient patient to reality if needed, do not confirm hearing voices or seeing nonexistent objects
Anger � remain calm, be open and honest, be supportive, do not belittle or provide false assurances, ensure your own safety
Children � be at eye-level, keep voice gentle, use slow movements, explain procedures, rephrase to ensure understanding, use play, understand if child reverts to lower developmental levels due to fear, allow expression of fear, assess situation with teens before including parent, do not judge
Grief � be empathetic, know Kubler-Ross� stages of grief, allow time for expression, use therapeutic touch, do not show pity
9. Elizabeth Kubler-Ross
10. Defense Mechanisms Mental devices used to feel more comfortable and make behavior seem
more reasonable to self and others; protect us from loss of self-esteem
Rationalization- offering a socially acceptable explanation for behavior when true reason is too painful; excuses
Projection � placing blame on someone else or attributing one�s own unfavorable characteristics or desires to someone else
Displacement � redirection of strong feelings about one person to someone else; taking feelings out on another person
Daydreaming � escape device of substituting fantasy for reality
Escape into Illness � using illness to be rewarded with attention or concern; learned behavior from childhood
Repression � forcing unpleasant memory into subconscious mind
Withdrawal � shutting off communication or removing oneself from a threatening situation
11. Roadblocks to Communication Belittling � making light of patient�s fears
Disagreeing � indicates belief that patient is incorrect
Defending � repelling a verbal attack
Stereotypes � statements that are not sincere; are biased and discriminatory
Changing the subject � prevents talking about topic that causes anxiety or fear
Reassuring clich� � insincere statement
Giving advice � shows you think you know what is best for patient or what they should do
Agreeing � shows patient�s message is correct even if not so, may not be real concern of patient
12. Positive Relationships Be a role model � earn trust of patients
Use professional communication � be respectful, use appropriate demeanor
Use proper forms of address � show respect, do not use pet names, use Mr. or Mrs. If applicable, use last names
Professional distance � do not become too personally involved, be objective, create therapeutic environment
Teaching patients � be knowledgeable of current medical trends, issues, etc.., be aware of special services, allow time, use quiet space, be clear, encourage questions, use open-ended questions, invite follow-up phone questions
Communicating with peers � be team player, avoid non-work related topics except on breaks, be honest
Communicating with physicians � be professional, use appropriate terms, address as Dr. unless told otherwise, use proper medical terms, be confident, admit mistakes, ask questions
Communicating with other facilities � maintain confidentiality, be professional, you represent your physician, observe legal requirements, facts only, do not judge, confirm messages are received