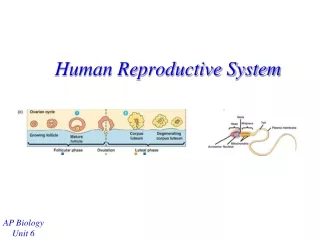
Human Reproductive Disorder
Human Reproductive Disorder. Xulan Dept. of G & O, the First Affiliated Hospital of Shantou University Medical College. Introduction of Infertility ※ Definition Fecund: the ability to reproduce, typically used in context of women to become pregnant.

Human Reproductive Disorder
E N D
Presentation Transcript
Human Reproductive Disorder Xulan Dept. of G & O, the First Affiliated Hospital of Shantou University Medical College
Introduction of Infertility ※ Definition • Fecund: the ability to reproduce, typically used in context of women to become pregnant. • Infertility: the inability to conceive after two years or more of trying with unprotected intercourse for couples. ( WHO, one year)
Primary infertility: no previous pregnancies have occurred • Secondary infertility: a prior pregnancy has occurred, but inability to conceive again for two or more years exposure to intercourse, no matter how the result of the pregnancy is.
What are the chances of a fertile couple actively seeking pregnant in a single month or cycle? 10%-20% • The accumulated pregnancy rate during two years __chances of conceiving by 6 months: 75% __chances of conceiving by 1 year:90% __10%-15%of couples will require longer than one year to conceive.
Epidemiology and etiology of infertility Causes Percentage Female factors 30-50 % Male factors 30 % Both male and female factors 20 % unexplained factors 10 % So, the initial evaluation should include both the partners.
※ Female Infertility • Causes • Ovulatory dysfunction: 25%. • Tubal factors: 30%-50% 3. Pelvic factors 4. Cervical factors 5. Extra-genital tract factors 6. Others
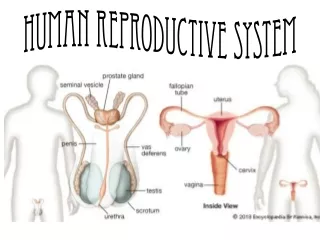
Female Factors Hypothalamus Pituitary Follopian tube Uterine ovary oocyte Cervix Extra-genital tract Fig.1sperm Thyroid Adrenal
Ovulatory dysfunction 1. Hypothalamus: amenarrhea or mensrtual disorder -- Emotional depress -- Psychological trauma -- Environmental and Climate changes 2. Pituitary diseases: --Sheehan’s syndrome -- Pituitary tumor: Hyperprolactinemia, -- Empty sella syndrome
Ovary diseases: 1. Congenital dysformation: Turner’s syndrome(45,XO) 2. Polycystic syndrom(PCO) 3. Premature ovary failure(POF) 4. Ovary functional tumors 5. Insensitive to follicle stimulating hormones(FSH). 6. Other endocrinologic diseases: adrenal or thyroid dysfunction
● Pelvic Factors Tubal factors: tubal blokage, adhension and hydrosalpinx 1. Inflammations --Chlamydia --Gonorrhea --Tubercle bacillus and so on 2. Tubal dysformation 3. Pelvic adhension: endometriosis 4. Abdominal or pelvic surgery 5. Ectopic pregnancy
●Pelvic factors Pelvic Adhension 1.Inflammations: --Chlamydia, turbercle bacillum, gonorrhea, staphylococci and so on 2. Pelvic endometriosis 3. Pelvic surgery ●Reproductive system dysformation -- Mayer-Rokitansky- Kuster-Hauser syndrome: no uterus and vagina
-- Uterus didelphys -- Uterus bicornis -- Uterus septus -- Uterus unicornis -- Rudimentary horn of uterus -- others
Fig.13-1 Fig.13-2
Cervical factors -- Cervicitis : cervical erosion, cervical polyps, cervical hyperplasia -- cervical stenosis -- Cervical tumors: leiomyoma -- Cervical cancer
●Extra-genital factors -- Vulvo-vaginalitis -- Vulvo-tumors ● Others --Immunological factors: autoimmune response; auto-antibodies: AsAb, ACA, ANA, etc. -- Genetic factors -- Psychological factors: -- Unexplained causes
Evaluation and diagnosis Initial evaluation The initial visit is the most important; the infertility is a problem of both of the couple; so, the male partner should be present at the beginning.
1. Taking history: -- marriage, menarche, menstruation -- duration of sexual relationships with or without birth control -- methods of birth control -- reproductive history of both partners (ie: children with previous partners/marriages)
2. Physical examination (PE) --General development -- Secondary sexual characteristics 3. Pelvic examination (PV) -- Bimanual exam -- Rectal-vaginal exam
4. Breast exam: masses and galactorrhea 5. Laboratory: -- hormonal testing: -- urinary LH surge test -- vaginal shedding cells test -- cervical mucus test -- post-coital sperm—cervical mucus test 6. Assisted imaging examination -- Ultrasound B continuous monitoring -- HSG -- Hysteroscopy -- Laparoscopy
Treatment for female fertility • General therapy -- Watchful waiting (provide more time for unassisted conception) -- more frequent intercourse at mid-cycle -- emotional support
2. Special therapy -- treatment of pelvic inflammation disease(PID) -- hydrotubation: -- selective salpingogram and recanalization: to make the obstructed site of the tube reopen under X-ray guidance -- hysteroscopy:removal of submucous leiomyoma, endometrial polyps, complete or incomplete uterus septum and separation of the cavity adhension. -- laparoscopy: adhension separation, ovarian tumors and leiomyoma removal
Surgical approaches: -- ovary cysts and tumors -- severe pelvic adhension -- Leiomyomas out of uterus wall • Physical treatment for cervical erosion: -- laser light -- crpyotherapy -- electrotherapy • Anti-tuberculosis: -- endometrial tuberculosis -- salpingotuberculosis.
Medication therapy • Ovulation induction • Clomiphene citrate(CC) M5 50-150mg qn×5 2. CC/HMG/HCG M5-9 CC 50-150mg M10-11 HMG 75IU qd 3. LHRH pulsive therapy 4. Bromocriptine---hyperprolactinemia 5. Metformin---PCO
6. HMG/HCG M3 HMG 75IU qd F 18-25mm, EN 8-10mm HCG10000IU qd ● Progesterone supplement 1. Post-ovulation, progesterone 10-20mg qd×7-10 days 2. HCG 2000IU-5000IUq3d82 3. Low dosage thyroid 20mg qd ● Assisted reproductive technology (not discussed here)
Methods to monitor ovulation -- Luteinizing Hormone monitoring: LH surge-- ovulation occurs after 34-36 hr, BBT--simple, cheap, biphasic pattern, -- Mid-luteal serum progesterone: > 15.7nmol/mL, peak; -- Premenstrual molimina: 95% presence, -- Mucus change: thick and cellular, no crystalline fern, -- Ultrasound monitoring: follicle size 21-23 mm, fluid in the cul-de-sac.
※ Male infertility • Causes 1. PRE-TESTICULAR CAUSES OF INFERTILITY a. Hypothalamic disease • Isolated gonadotropin deficiency (Kallmann's syndrome) • Isolated LH deficiency ("Fertile eunuch") • Isolated FSH deficiency Congenital hypogonadrotropic syndromes
b. Pituitary disease • Pituitary insufficiency (tumors, infiltrative processes, operation, radiation) • Hyperprolactinemia • Hemochromatosis • Exogenous hormones (estrogen-androgen excess, glucocorticoid excess, hyper and hypothyroidism).
2. TESTICULAR CAUSES OF INFERTILITY • Chromosomal abnormalities: Klinefelter's syndrome (XXY, karayotype), XX disorder (sex reversal syndrome), XYY syndrome • Noonan's syndrome (male Turner's syndrome) • Myotonic dystrophy- Bilateral anorchia (vanishing testes syndrome) • Sertoli-cell-only syndrome (germinal cell aplasia)
Gonadotoxins (drugs, radiation) • Orchitis • Trauma • Systemic disease (renal failure, hepatic disease, sickle cell disease) • Defective androgen synthesis or action • Cryptorchidism • Varicocele
3. POST-TESTICULAR CAUSES OF INFERTILITY a. Disorders of sperm transport ● Congenital disorders ● Acquired disorders ● Functional disorders b. Disorders of sperm motility or function ● Congenital defects of the sperm tail ● Maturation defects ● Immunologic disorders ● Infection 3. Sexual dysfunction
● Evaluation and diagnoses 1.History collection: -- period of infertility without protected intercourse -- present and previous marriage, -- previous fertile history with partners, -- frequency of intercourse, -- method of birth control, -- harmful habits: cigarette, alcohol, drug-injection
2. Physical examination -- development of body: height and ratio of upper body sigment to low body sigment -- Secondary sexual characteristics Inadequate body hair atypical genital hair distribution gynecomastia
-- Exam of reproductive system Size, masses (length, volume and mass) of scrotum Use orchidometer if possible Epididymis for scarring ,absence or induration Vas deferense for absence or nodules Varicocele 3. Laboratory test -- Semen analysis -- Karyotype (chromosome)
Normal Values for Semen Analysis Volume > 2.0 mL Sperm concentration > 20 million/mL Motility >50 % A >25% A+B >50% morphology >30 % normal Data from WHO, 1992