Download
1 / 29
370 likes | 2.03k Views
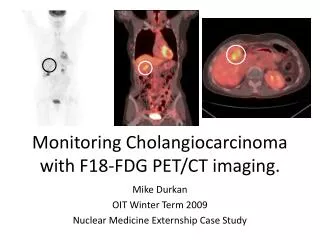
Cholangiocarcinoma Clinics in Liver Disease- Volume 12, Issue 1( February 2008). Clinical Journal of Oncology Nursing-Volume 5, Number 4‧Cholangiocarcinoma: A Nursing Perspective. NP 張正玉 971103 Cholangiocarcinoma( CC): Introduction

E N D
CholangiocarcinomaClinics in Liver Disease- Volume 12, Issue 1( February 2008).Clinical Journal of Oncology Nursing-Volume 5, Number 4‧Cholangiocarcinoma: A Nursing Perspective. NP張正玉 971103
Cholangiocarcinoma( CC):Introduction • It’s the second most common primary hepatic neoplasm in adult.(盛行率:約為HCC的1/10) • It’s incidence has increased within the last 3 decades without clear etiologic explanations. • The majority of patients are over 65 years of age; men and women are affected in equal proportion.
Risk factors for CC • Primary sclerosing cholangitis • Congenital biliary cystic disease • Ulcerative colitis • Hepatolithiasis • Biliary parasites(中華肝吸蟲, Opisthorchis viverrini) • Radionuclides (thorium釷、radon鐳) • Chemical carcinogens( dioxin、石棉、四氯化碳、多氯聯苯、DDT、染料等)
Types of CC CC can occur anywhere on the biliary tree, from the ampulla of Vater to the IHD. • Intrahepatic CCs( peripheral ):usually present as a solitary mass in the liver.(6-10% of all cases of CC) • Extrahepatic CCs • Hilar (klastkin):40-60% of all cases of CC • Mid CCs: 17-20% • Distal CCs: 20-30%
Clinical presentation • Most CCs remain clinically silent until the advanced stage. • Extrahepatic CC: • Initial symptoms are vague. • Jaundice(75~90%): when biliary flow to duodenum is blocked. • Acholic stool, pruritus • Weight loss, abdominal pain, occasional fever( cholangitis).
Clinical presentation • Intrahepatic CC: • Jaundice is not common. • Usually present with RUQ pain. • Other symptoms, often vague, include weight loss or intermittent fevers. • Cachexia and malaise.
Clinical evaluation • Imaging studies are used to determine the level of biliary obstruction and hepatic involvement and to assess for vascular invasion or metastatic disease. • Ultrasonography • Computed tomography • Magnetic resonance cholangiopancreatogram • Endoscopic cholangiogram • Percutaneous transhepatic cholangiography
Ultrasonography • Non-invasive • Uses sound waves to determine the level of biliary obstruction, hepatic involvement and overall extend of disease. • Operator dependent • Sensitivity and specificity is poor in the diagnosis of CC, and staging relies on other imaging modlities.
Computed tomography • Helpful in the staging, pre-op planning, and evaluation of vascular encasement. • Hilar tumor masses are difficult to visualize by CT. • Evaluation of intraductal spread and detection of lymph nodes and peripheral metastasis by CT is suboptimal.
Cholangiography • MRCP is the best imaging modality for CC. • Provides information about tumor extend, biliary and hepatic parenchymal anatomy, and intrahepatic metastasis. • Non invasive • Distal extrahepatic CC is optimal evaluated byERCP. • PTC and ERCPallow bile duct sampling for diagnostic analysis and stents insertion.
Angiography • It shows the anatomical location of hepatic artery and portal vein. • To evaluate the resectability.
Lab analysis • Basic BCS: albumin, bilirubin( T/D), AST, ALT, alkaline phosphatase and total protein. • Tumor marker: CEA 及CA19-9 之升高不具診斷意義 • Cytology analysis: • Obtained by brush cytology or bile duct biopsy during ERCP. • Percutaneous biopsy of the primary tumor is not advised.( tumor spread)
Treatment criteria • Based on the location and extent of the tumor, distant disease, comorbidity and cirrhosis. • Potentially curative treatment: surgery! • Goal of surgery: complete excision of the tumor with negative histologic margins and biliary reconstruction. • Palliative : surgical biliary- entric bypass, biliary endoprosthesis, C/T, R/T, photodynamic therapy and supportive care.
Prognosis • Poor ! • The prognosis varies based on resectibility and anatomical location of tumor. • Average survival time is approximately 14 months. • The mean survival for patients with unresectable lesions is 6-12 months.
Prognosis • Hilar tumor: untreated CC→ less then 12 months, resection is possible for only 1/3 of patients. • Distal and mid tumors: unresectable CC→ 6~ 12 months, after resection→ 16~33 months. • Intrahepatic CC: unresectable CC→7 months, undergo surgical resection→ 44~59 months.
Treatment modalities-Potentially curative surgical procedures • Hilar (Klatskin) tumor : • bile duct excision+ biliary reconstruction, partial hepatectomy usually is required. • Mid and distal CC: • Early, localized ca(少數): wide, local duct excision. • Whipple operation • Intrahepatic CC: partial hepatectomy
Treatment modalities- Palliative interventions • Biliary decompression • To palliate associate symptoms: jaundice, pruritus and cholangitis. • Surgical biliary- enteric bypass: for patients with unresectable disease • Disadvantages: they are major operative procedures with associate morbidity.
Complications of surgical intervention • Biloma • Abscess formation • Liver failure after partial hepatectomy • Renal insufficiency resulting from liver failure • Biliary obstruction • Wound infection • Cholangitis
Nonsurgical palliative procedure • Percutaneous • An internal / external catheter + bag or internal metal stent is used for biliary decompression. • At times, multiple stents are reguired to obtain adequate drainage. • Endoscopic • Is able to see the biliary ducts and place the biliary endoprothesis( plastic/ metallic stent) • Plastic: occlude easily, change every 2-3mons • Metallic: offer a long period of patency , but not removable or exchangeable.(用於存活>6個月) • Complication: cholangitis
Other palliative treatment modalties • Chemotherapy: limited! No proven role in the treatment of CC. • Radiation: No benefit or increase in survival time. • Photodynamic therapy: inject photosensitive agent to the body→appropriate light wave to produce tumor cell death via cholangioscopy→ biliary decompression. • Best supportive care: • Treat the patient symptomatically( pain, ascites, anorexia, and jaundice with pruritus). • Comfort is the goal! • Psychosocial support also is essential.
Pre- and postoperative care • Preoperative care • Patient education materials. • Questions are encouraged and answered, and emotional support is provide. • Postoperative/ postprocedure care • Vital signs, pain, intake and output monitoring • CBC, BCS+e-, PT QD for 3days, then QW1,4 • During liver regeneration, PT↑: FFP and Vit.K • Check wound daily, patient are encouraged to take daily showers. • Assess their condition over the phone after discharge.
Management of complications • Cholangitis:administration of antibiotics, antipyretics, monitoring of vital signs • Bilomas/ abscess:PTCD drainage→ catheter care • Wound infection:assessment of skin integrity frequently, wound care/ wet dressing if needed • Pneumonia:aggressive pulmonary toilet, frequent ambulation • Liver failure: encephalopathy, fatigue, renal insufficiency,→ low protein diet, Lactulose side effect, appropriate activities.
Palliative care • Encourage them to verbalize their feelings! • Educate them about hospice care and the dying process. • Ascites and leg edema: diuretics, e- levels and renal function monitoring, low sodium diet, daily weights, and paracentesis care. • Pruritus: lotion for skin, tepid oatmeal baths, cold packs. • Assess tolerance of the diet: small, frequent meals and snacks, appetite stimulants, nutritional supplement.( Bile salt deposit on the tongue→ taste change)
Summary • Cholangiocarcinoma is a highly malignant tumor and the second most common form of primary hepatic carcinoma. • The mean survival for unresectable lesions is 6~12 months. • Surgical resection is the only treatment modality that offer a potential cure and prolonged survival. • Nurses work with physicians and hospice team to coordinate pain management, infectious complications, biliary drain management, and terminal care.
Photodynamic treatment • PDT uses laser, or other light sources, combined with a light-sensitive drug (sometimes called a photosensitising agent) to destroy cancer cells. • A photosensitising agent is a drug that makes cells more sensitive to light. Once in the body, the drug is attracted to cancer cells. It does not do anything until it is exposed to a particular type of light. When the light is directed at the area of the cancer, the drug is activated and the cancer cells are destroyed. Some healthy, normal cells in the body will also be affected by PDT, although these cells will usually heal after the treatment.
How PDT is given • Stage 1: A light-sensitive drug is given. For cancers of the skin, the drug is usually applied to the skin as a cream. • For cancers that are inside the body, the drug is usually given by injection into a vein (intravenously). There are some drugs that can be given by mouth. • There is a delay between the cream being applied, or the drug being given, and the next stage of treatment. This allows time for the drug to concentrate in the cancer cells. • Stage 2 :involves shining light directly on to the cancer. A laser delivers energy in the form of light in a very precise way. Special non-laser lamps may also be used in some situations. • For skin cancers, the light is shone directly onto the skin. • For internal cancers, a flexible tube (an endoscope) may need to be passed into your body to deliver the light to the tumor.