Download
1 / 22
370 likes | 1.26k Views
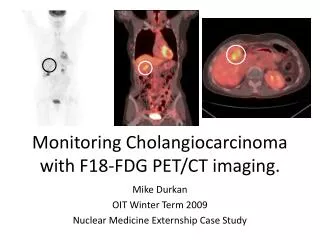
Monitoring Cholangiocarcinoma with F18-FDG PET/CT imaging. Mike Durkan OIT Winter Term 2009 Nuclear Medicine Externship Case Study. Contents. Introduction---------------------------------------- 3 F18 FDG---------------------------------------------- 4

E N D
Monitoring Cholangiocarcinoma with F18-FDG PET/CT imaging. Mike Durkan OIT Winter Term 2009 Nuclear Medicine Externship Case Study
Contents Introduction---------------------------------------- 3 F18 FDG---------------------------------------------- 4 PET/CT Procedure--------------------------------- 5-9 Cholangiocarcinoma------------------------------10-13 FDG PET and CCC----------------------------------14-18 NOPR-------------------------------------------------19 NOPR: Proposed Coverage----------------------20 Conclusion------------------------------------------21 References------------------------------------------22
Introduction In 2005 under Medicare’s Coverage with Evidence (CED) program the National Oncologic PET Registry was created. “The NOPR is a collaboration of the American College of Radiology Imaging Network (ACRIN), the American College of Radiology (ACR), and the Academy of Molecular Imaging (AMI), to ensure access to Medicare reimbursement for certain types of positron emission tomography (PET) scans.” The creation of the NOPR allows future reimbursement options to be developed from evidence based data and research. Recently , on January 6, 2009, a group of physicians submitted a 24 page memorandum that proposed a changed in current Medicare reimbursement coverage for FDG PET oncological indications. The change would make FDG PET a stronger tool in the management of cancer. With this change new cancers and new coverage options would expand the diagnostic use of FDG PET. One cancer with proposed changes in coverage was Cholangiocarcinoma. On January 19th, 2009, I performed a PET/CT study on a 44yr old female that had a history of Klatskins tumor a Perihilar Cholangiocarcinoma. Due to the pathophysiological nature of this cancer and level of tumor growth, surgical resection was unable to completely remove the tumor. Malignant cells still remained in the biliary tract and surrounding tissue. To further evaluate the level of malignant tumor growth and assess treatment options the oncologist used PET/CT imaging. This case study will describe the FDG PET/CT procedure, the pathophysiology of Cholangiocarcinoma, and how FDG PET/CT benefits patients with this disease.
F18 FDG F18 FDG • F18 FDG (flurodeoxyglucose) is a nonorganic analog of the organic molecule glucose. • F18 is produced via duetron bombardment of Neon-20 or proton bombardment (p,n) of Oxygen-18 in a medical cyclotron. (the latter is most often used). • T1/2= 110 minutes • The annihilation of positronium (a positron and electron) produces two 511 keV photons that travel 180° degrees apart. • F18’s mean positron range is 0.2mm with a maximum range of 2.4mm. This is an ideal range for PET resolution. • F18 FDG is actively transported through cellular membranes where the enzyme hexokinase transforms the molecule into FDG-6-phosphate. Once FDG-6-P is produced in the first step of glycolysis, the molecule permanently remains in the cellular cytosol. Glucose
PET/CT Procedure MATERIALS • 1x Butterfly needle. • 1x Three way stopcock • 2x 10cc syringe w/saline (15%NaCl in 10ml sterile H₂O) • 1x Tungsten PETPig™ • 21mm (7 half value layers) • 20oz solution of 50%H₂O and 50% Barium oral CT contrast • 1x Positive pressure cap
PET/CT Procedure EQUIPMENT • GE Discovery ST PET/CT scanner. • Xeleris Hawkeye PET/CT processing module • Bismuth germanate (BGO) scintillation crystal. • BGO cut-block detector • 7.1gm/cm³ • 300nsec Decay time • 2D tungsten detector configuration • 6 or more table positions.
PET/CT Procedure PATIENT PREPARATION • Fasting for 6-8 hours prior • Physical activity is restricted • Meals low in carbohydrates and high in protein and lipids are recommended. • To reduce cardiac FDG uptake, Doctors want the heart to be processing fats into energy. • Blood Glucose levels are taken from patients with Type I and II Diabetes. • Patients with Type I or Diabetes Mellitus continue normal management of Blood glucose levels. • Prior studies and Patient histories are brought either on film, CD, or paper. • Most patients are referred from Fairbanks, Nome, and other regions in Alaska. The Radiologists need a firm patient history and comparative image studies to evaluate prior, initial, and future diagnostic imaging.
PET/CT Procedure INJECTION • Blood Glucose levels are checked only if the patient recently ate or the patient has diabetes. • Patient anxiety and claustrophobic issues are allayed by administering 0.5mg aprazolam (Xanax) one hour before imaging. Patient transportation after the study must be supplied by a significant other or taxi service • IV access is established with a Butterfly and Three way stopcock. • The F18 FDG dose is then assayed and brought into the room. • A small volume of saline is flushed through the IV to ensure patency. • The dose is injected and followed by 20 cc Saline. • The patient’s 1 meter radiation dose rate is about 1mrem/hr so the patient remains in the lead shielded injection room for 45 minutes to 1 hour. • To reduce brown fat uptake, warm blankets are supplied and the room’s temperature is kept warm.
PET/CT Procedure ACQUISITION & PROCESSING • The patient is positioned supine, head first with their arms above their head. • Metallic objects, false-teeth, and prostheses are removed from the field of view. • The CT consists of an 8 slice 25 second scan from the orbitomeateal line through the pelvis. The average table length is 75cm. Sometimes scan length is extended to accommodate taller patients. • 2D PET acquisition allows for less computer processing and larger camera bores to prevent claustrophobia. • The PET acquisition averages 24 minutes with 6 bed stations. • Lung specific PET/CT studies are acquired after limited whole body scans to better differentiate Lung parenchyma and changes in FDG localization. • Some lung cancers, especially non-small cell carcinoma, accumulate FDG over time. • After acquisition the images are assessed for motion and attenuation accuracy. • Before the data is displayed the computer automatically applies an MLEM and OSEM HANN reconstruction algorithm. • The RAW PET/CT data is sent to the Advantage DICOM 4.3 workstation where the fused data is displayed in the sagittal, transverse, coronal planes. • The DICOM 4.3 and Dr. Xeleris workstation allows Radiologists to use quantitative image analysis with Body weight and Body surface area Standard uptake values (SUV).
Cholangiocarcinoma • Cholangiocarcinoma (CCC) has two subtypes with ancillary groupings: • Perihilar: (70-85%)Most common form of cholangiocarcinoma that is usually a highly desmoplastic (fibrous) adenocarcinoma. • Peripheral • Hilar (Klatskins tumor) • Intrahepatic: (20-25%) This form usually grows as a mass around the biliary tract in the liver • 1/100,000 chance of developing CCC. • 6 month survival rate for overall patient population. • Unknown etiology. Some conditions are suspected to increase a person’s risk of developing CCC. Research shows a correlation between Primary Sclerosing Cholangitis (PSC).
Cholangiocarcinoma • Perhilar CCC, Klatskin tumor and Peripheral CCC, are commonly found at the bifurcation of the Left and Right Hepatic bile ducts (extrahepatic). • Perihilar CCC also develops in the intrahepatic bile ducts. • The desmoplastic nature causes the cancer to be mistaken for other cancers (HCC, pancreatic cancer metastases, and gallbladder cancer). • Perihilar and Intrahepatic CCC are diametrically different; gentically and histiologically. • Perihilar is easier to identify with CT, MRI, and ERCP (Endoscopic Retrograde Cholangipancreatography). CT is also used to monitor the tumor’s mass over time
Cholangiocarcinoma Bismuth-Corlette STAGING • Oncologists commonly use the American Joint Committee on Cancer Guidelines (AJCC) tumor, node, and metastasis (TNM) scale to classify tumor pathology. • Surgeons use the Bismuth-Corlette classification to further evaluate tumor resectability and required procedures. • Physiologically, Perihilar and Intrahepatic CCC present with conspicuous symptoms. Physical symptoms often present in late stages of tumor growth. • 50% of patients have lymph node involvement at initial diagnosis (Stage III). 10-20% have peritoneal involvement. • Treatment options usually consist of tumor resection, however most tumors are desmoplastic formations around the hilum and unresectable at diagnoses
Cholangiocarcinoma Diagnostic Approach for Cholangiocarcinoma MR and CT imaging PET Scan
FDG PET and CCC • Medicare's establishment of the NOPR allowed new cancers to be imaged with F18-FDG. • CCC was one of the cancers the NOPR provided CED reimbursement for. • This platform allowed physicians to research the impact of FDG PET imaging in CCC. • One article claimed FDG F18 imaging was 92% sensitive and 93% specific for detecting CCC. This finding includes Perihilar and Intrahepatic CCC. • No research has been done on the diagnostic significance of FDG F18 imaging to prevent CCC. Current studies have been developed around staging, treatment options, and monitoring CCC. • Compared to MRI, ERCP, CT, and US; FDG PET imaging is more sensitive in identifying distant metastases in CCC and can differentiate between Primary Sclerosing Cholangitis (PSC), a benign condition of the biliary system. CCC and PSC are structurally similar and can be mistaken for each other.
FDG PET and CCC IMAGE ARTIFACTS • According to the Bismuth-Corlette classification scheme for Klatskin CCC adenocarcinomas, patients with Type I-IV receive a hepaticojejunostomy (biliary stent). Some FDG PET studies show false uptake from these structures making it difficult to discriminate between tumor uptake and biliary stent uptake. • The patient imaged had a known plastic biliary stent that showed little FDG activity compared to tumor activity. • Kluge et al. suggests normal SUV quantitative values may produce inaccurate grading of tumor activity. The semi quantitative T/N (tumor/non-tumor) grading scales are better for FDG PET imaging in CCC. • Tumor size may limit FDG accumulation and produce a false negative in early detection. • Cholangitis and inflammation from other hepatobiliary diseases that commonly occur comorbidly with CCC can produce false FDG accumulation.
FDG PET and CCC October SUV=3.5 grams/ml. • The patient imaged on January 19th had a previous PET/CT study in October ‘08. The FDG PET studies were used to monitor Klatskin tumor growth. • According to the TNM grading scale the patient had stage III CCC and was treated with a variety of procedures. • The patient underwent tumor resection and other major surgical interventions to remove the tumor. The Bismuth-Corlette scheme showed a Type IV tumor. • Following experimental treatment with Xeloda, a chemotherapy drug, the patient’s cancer was restaged with a PET/CT and Abdomen CT. • Three non-enlarged lymphnodes in the mediastinum showed increased FDG accumulation. • The Radiologist used Qualitative comparisons with Standard Uptake Values for patient weight. SUVs greater than 2.5-3 grams/ml are considered abnormal. January SUV=5.7 grams/ml.
FDG PET and CCC January ’09: PET Fused with Mediastinal Lymphnode metastases • The January ‘09 image shows two non-enlarged mediastinal lymphnodes with increased activity with a maximum SUV of 4.6 grams/ml. • The SUV value was correlated with previous mediastinal lymphnode values recorded in October to rule out benign activity. • The Second image shows the initial diagnoses of Klatskins tumor with an Abdomen Pelvis CT study performed in 2005. • The patient’s physical symptoms, liver enzyme labs, and other antigen specific blood tests further indicated CCC. • The tumor’s location and growth indicated a CCC Klatskin tumor. September ’05: CT showing initial Klatskins tumor
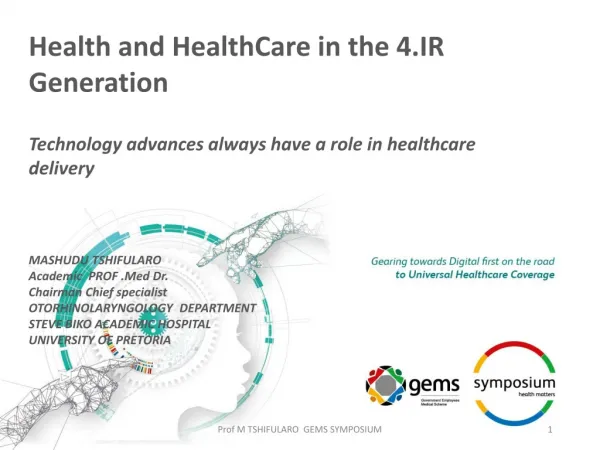
FDG PET and CCC January ‘09: This image set shows fused PET/CT transverse 8.82mm slices from SuperiorInferior. Notice the FDG uptake in the central part of the liver RT LT
NOPR • The National Oncologic PET Registry (NOPR) allows patients to receive free diagnostic testing for national research purposes. • With the data collected over that last four years and current proposals for Medicare reimbursement changes, FDG PET imaging will allow more accurate diagnostic data to the management of cancer. • The management of CCC is just one cancer that has been shown to benefit from FDG PET imaging. • Later this month the Medicare Evidence Development & Coverage Advisory Committee (MedCAD) will release its finial decision regarding the proposed changes. • Following this slide is a list of proposed changes from current coverage.
Proposed NOPR PET/CT Medicare Reimbursement Coverage *CED: Coverage with Evidence Development
Conclusion The main purpose of this case study was to show how FDG PET imaging can benefit the management of cancer, specifically CCC. Without utilization of this technology and established databases like the NOPR, management of CCC in the mentioned patient’s care may have been limited or demanding. Although FDG PET in CCC management is a narrow example of NOPR data collection, this shows the level of opportunities offered through this organization and the discernment used to find newer more advanced non-invasive procedures. Over time, as more NOPR CED studies are submitted and more data is collected, coverage entities may provide broader plans to compensate for changes in FDG PET imaging in the management of disease.
References Hillner, Bruce E., Siegel, Barry A., Liu, Dawei, & Shields, Anthony F. (2008). Impact of Positron Emission Tomography/Computed Tomography and Positron Emission Tomography (PET) Alone on Expected Management of Patients With Cancer: Initial Results From the National Oncologic PET Registry. Journal of Clinical Oncology, 26, 1155-1161. Kieding, Susanne, Hansen, Soren B., & Rasmussen, Henrick H. (1998). Detection of Cholangiocarcinoma in Primary Sclerosing Cholangitis by Positron Emission Tomography. Hepatology. 28, 700-706. Kluge, Regine, Schmidt, Frank, & Caca, Karel (2001). Positron Emission Tomography With [18F]Fluoro-2-deoxy-D-glucose for Diagnosis and Staging of Bile Duct Cancer. Hepatology. 33, 1029-1035. Gores, Gregory J. (2003).Cholangiocarcinoma: Current Concepts and Insights. Hepatology. 37, 961-969. Hillner, Bruce E., Siegel, Barry A., & Liu, Dawei (2008). Relationship Between Cancer Type and Impactof PET and PET/CT on Intended Management:Findings of the National Oncologic PET Registry. Journal of Nuclear Medicine. 49, 1928-1935. Gores, Gregory J (2000).Early Detection and Treatment of Cholangiocarcinoma. Hepatology. 6, S30-S34. Bismuth, Henri (1992).Management Strategies in Resectionfor Hilar Cholangiocarcinoma. Annual Journal of Surgery. 215, 31-38. Khan, S. A., Davidson, B. R., & Goldin, R Guidelines for the diagnosis and treatment ofcholangiocarcinoma: consensus document. British Journal of Medicine, 51, Retrieved March 2, 2009, from http://gut.bmj.com/cgi/content/full/51/suppl_6/vi1. Darwin, Peter E. (2008). Cholangiocarcinoma. In EMedicine [Web]. Medscape. Retrieved March 2, 2009, from http://emedicine.medscape.com/article/277393-overview Reihnhart, M. J., Strunk, H., & Gerhart, t. (2005). Detection of Klatskin’s Tumor in Extrahepatic Bile Duct Strictures Using Delayed 18F-FDG PET/CT: Preliminary Results for 22 Patient Studies. Journal of Nuclear Medicine. 46, 1158-1163.