Download
1 / 13
150 likes | 633 Views
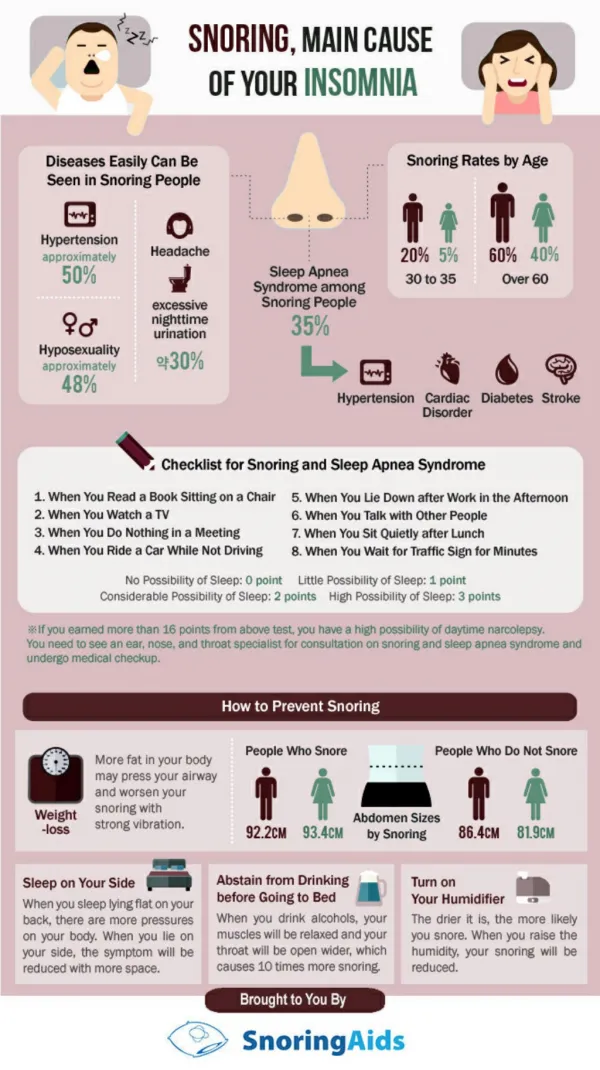
Snoring basics. Common15-20% of children60% 60 year old men 40% 60 year old womenDirectly related to BMIMost common exacerbating factor is alcohol. Snoring basics 2. Vibration of the upper airwaysInspirationCollapse of the upper airwayA minority of cases caused by nasal obstructionVery rarely caused by unusual pathologySevere snorers may have obstructive sleep apnoea (OSA).

E N D
1. Management of snoring John Waldron
15 October 2008
2. Snoring basics Common
15-20% of children
60% 60 year old men
40% 60 year old women
Directly related to BMI
Most common exacerbating factor is alcohol
3. Snoring basics 2 Vibration of the upper airways
Inspiration
Collapse of the upper airway
A minority of cases caused by nasal obstruction
Very rarely caused by unusual pathology
Severe snorers may have obstructive sleep apnoea (OSA)
4. Snoring basics 3 In patients with a BMI in the normal range vibration of the soft palate and uvula is the most common cause
In overweight patients multi level collapse of the pharyngeal airway due to sub mucosal adipose tissue narrowing is common
5. Obstructive sleep apnoea Breathing stops due to complete collapse of the airway
Period of silence, may last 30 seconds or more
Frequency of episodes is a measure of severity
May wake the patient
Prevents them reaching deeper (REM) �restorative� sleep levels
Wake feeling unrefreshed, headache, hypersomnolence, tiredness, accidents, reportable to the DVLA
May lead to cardiac problems in severe cases
6. Snoring history How long
How often
Time course
Positional
Consequences for the partner, patient, others
History of apnoea, patient waking, quality of sleep, hypersomnolence (Epworth)
7. Snoring history 2 BMI
Weight change over time and relationship to snoring
Collar size
Nasal obstruction
Smoking
Alcohol intake, timing, and relationship to snoring
8. Snoring examination Mouth including soft palate and tongue
Jaw (retrognathia)
Nasal airway
Nasendoscopy
NE with forced inspiration
NE with forced snoring
Measure BMI
9. Snoring investigations Sleep study if concern about significant sleep apnoea
If doubt about frequency/length of apnoeas ask partner to observe
10. Snoring treatment Is treatment necessary?
Earplugs
Sleeping position
Separate rooms
Stop smoking
Alter alcohol intake
Treat nasal obstruction with topical steroid or topical/systemic decongestant
11. Snoring treatment 2 Treat nasal obstruction which is significant on its own with medical treatment or surgery
Weight reduction
12. Snoring treatment 3 Mandibular advancement splint � can be tried in any patient
CPAP for patients with significant sleep apnoea
Surgery can be considered in patients who do not have significant sleep apnoea
13. Surgery for snoring Trimming of soft palate +/- tonsillectomy
Laser/electrocautery/microfrequency
Much less successful in significantly overweight patients
Much less successful in patients with significant sleep apnoea
Painful, small risk of significant complications with speech and swallowing