Download
1 / 20
250 likes | 1.01k Views
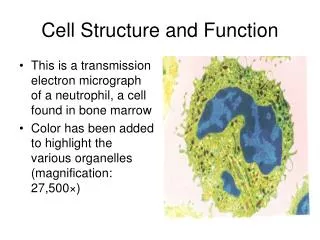
Bone Metastases In Renal Cell Carcinoma: What Can Be Done?. Fred Saad, MD, FRCS Director of Urologic Oncology Professor of Surgery/Urology U of M Chair in Prostate Cancer University of Montreal. Renal Cell Cancer: Background. More than 100,000 deaths per year worldwide

E N D
Bone Metastases In Renal Cell Carcinoma: What Can Be Done? Fred Saad, MD, FRCS Director of Urologic Oncology Professor of Surgery/Urology U of M Chair in Prostate Cancer University of Montreal
Renal Cell Cancer: Background • More than 100,000 deaths per year worldwide • Incidence steadily increasing over the past 3 decades • Many patients with renal cell cancer will develop bone metastases Ries et al. SEER Cancer Statistics. At: http://seer.cancer.gov/csr/1973_1999/. Accessed 2002. Zekri et al. Int J Oncol. 2001;19:379.
Bone Metastases in Renal Cell Cancer • The skeletal morbidity rate among patients with renal cell cancer during the first year was similar to that observed in patients with breast cancer and multiple myeloma (2.5 - 4.0 SREs/patient/year) • Bone metastases rarely respond to immune based therapy • Median survival of patients with bone mets: 12 months Zekri et al. Int J Oncol. 2001;19:379.
Renal Cell Cancer: Radiologic Appearance of Bone Lesions Among patients with bone lesions, the majority were osteolytic Zekri et al. Int J Oncol. 2001;19:379.
Renal Cell Cancer: Distribution of Bone Metastases No. of Patients (%)Site (n=31) Pelvis15 (48) Ribs15 (48) Spine13 (42) Femora 7 (23) Humeri 3 (10) Skull 3 (10) Clavicle2 (6) Ulna1 (3) Tibia1 (3) Zekri et al. Int J Oncol. 2001;19:379.
Renal Cell Cancer: Skeletal-Related Events No. of patients (%) No. of SRE (N=31) events Radiotherapy 25 (81) 37 Long-bone fractures 13 (42) 15 Hypercalcemia 9 (29)* 16 Orthopedic surgery 9 (29) 12 Spinal cord compression 4 (13) 4 *An additional 32 patients developed hypercalcemia without evidence of metastatic bone disease on imaging tests. Criteria for hypercalcemia not defined. Zekri et al. Int J Oncol. 2001;19:379.
Zoledronic Acid inPatients With Renal Cell Carcinoma and Bone Metastases Long-Term Analysis (21 Months)
Zoledronic Acid in Solid Tumors: Trial Design* R A N DO M I Z E D n=257 Zoledronic acid 4 mg q3wk n=250 Placebo q3wk 0 9 monthsCore analysis 21 months Final analysis
Efficacy Analysis • Primaryefficacyendpoint • Proportionofpatientsexperiencing≥1SRE • Pathologicbonefracture • Radiationtherapytobone • Spinalcordcompression • Surgerytobone • Secondaryefficacyendpoints • TimetofirstSRE • Skeletalmorbidityrate • Timetoprogressionofbonemetastases SRE = skeletal-related event; HCM = hypercalcemia of malignancy.
Tumor Types Tumor Type No. of Patients (%) NSCLC378(49) Renalcellcarcinoma74*(10) Smallcelllungcancer58(8) Colon/rectal/intestinal55(7) Cancerunknownprimary51(7) Bladder32(4) Esophagus/gastroesophageal17(2) Headandneck17(2) Melanoma16(2) Thyroid11(1) Othertumortypes(n=11)57(7) *Zoledronic acid 4-mg group and placebo (n=46). Rosen et al. J Clin Oncol. 2003;21:3150.
Proportion of Patients With Any SRE Zoledronic acid significantly reduces the proportion of RCC patients with an SRE P=0.011 100 79 80 60 RCC patients with any SRE (%) 41 40 20 0 Zol 4 mg Placebo (n=27) (n=19)
Time to First Skeletal-Related Event Zoledronic acid significantly extends the time to first SRE • Median No. of DaysP Value • Zol 4 mg4240.006 • Placebo72 Zol 4 mg27127421 Placebo1941100 *After start of study drug.
Percent of Patients With Each SRE Zoledronic acid consistently reduces all types of SREs
Time to Progression of Bone Lesions Zoledronic acid significantly extends the time to disease progression • Median No. of DaysP Value • Zol 4 mg5860.014 • Placebo89 Zol 4 mg27137320 Placebo1930000 *After start of study drug.
Time to First Pathologic Fracture Zoledronic acid significantly extends time to first pathologic fracture 100 • Median No. of DaysP Value • ZolNR0.003 • Placebo168 80 60 RCC patients without pathologic fracture (%) 40 20 0 0 120 240 360 480 600 * Days Zol 4 mg27179542 Placebo1961111 *After start of study drug.
Survival • Median No. of daysP Value • Zol 4 mg3470.104 • Placebo216 Zol 4 mg2723151182 Placebo19148521 *After start of study drug.
Andersen-Gill Multiple Event Analysis 58% reduction in the risk of developing an SRE for patients receiving zoledronic acid compared with placebo HazardRatio RiskReduction P Value 0.69 Lung and other solid tumors 31% 0.003 0.42 Renal cell cancer 58% 0.010 0 0.2 0.4 0.6 0.8 1 1.2 1.4 1.6 1.8 2 Relative risk In favor of placebo In favor of zoledronic acid
Hematuria2 (11.1)1 (6.7) Blood creat increased0(0.0)0(0.0) Hyperuricemia1 (5.6)0 (0.0) Renal failure1 (5.6)0 (0.0) Difficulty in micturition0 (0.0)1 (6.7) Oliguria0 (0.0)1 (6.7) Total 4 (22.2) 3 (20.0) Most Frequent Renal-Related Adverse Events* No. of Patients (%)† Zol 4 mg Placebo (n=27)(n=19) *Post 15-minute infusion; †Safety-evaluable population; ‡>0.5 mg/dL if baseline <1.4 mg/dL; >1.0 mg/dL if baseline >1.4 mg/dL.
Zoledronic Acid in Patients With Renal Cancer: Clinical Summary • Significantly reduced the proportion of patients with an SRE • Significantly decreased mean skeletal morbidity rate of all SREs • Extended time to first SRE and time to first fracture • Significantly increased median time to progression of bone lesions • Was safe and well tolerated
Bone Metastatic Renal Cell Carcinoma: Conclusions • New treatment options now available for metastatic RCC increase survival and may increase the time patients are at risk for bone comlications • Zoledronic acid can be considered a treatment option for patients with bone metastases from renal cell carcinoma