Download
1 / 14
150 likes | 818 Views
Hard Palate Necrosis after Bilateral Internal Maxillary Artery Embolization for Epistaxis. Joel Guss, Marc Cohen, Duane Sewell, Natasha Mirza Department of Otorhinolaryngology-Head and Neck Surgery University of Pennsylvania and The Philadelphia VA Medical Center. Case Report.

E N D
Hard Palate Necrosis after Bilateral Internal Maxillary Artery Embolization for Epistaxis Joel Guss, Marc Cohen, Duane Sewell, Natasha Mirza Department of Otorhinolaryngology-Head and Neck Surgery University of Pennsylvania and The Philadelphia VA Medical Center
Case Report • 50 year-old male admitted with severe hypertension • History of substance abuse, mechanical aortic valve replacement on Coumadin, renal failure on hemodialysis. • Started on a Heparin drip and develops right posterior epistaxis
Case Report • Continues to bleed despite placement of a 10 cc nasopharyngeal balloon pack and bilateral anterior-posterior nasal tampons • FFP given to correct coagulation parameters • 2 units packed red blood cells transfused • Referred to Neurointerventional Radiology – bilateral internal maxillary arteries embolization
Case Report • Nasal and nasopharyngeal packs removed 48 hours after embolization • No further bleeding, anticoagulation resumed • Over next week patient complains of right sided facial and oral pain
Discussion • Selective embolization of external carotid artery branches is safe and effective in treating epistaxis refractory to conservative management • Early success rates 71-100% in controlling hemorrhage
Discussion • Neurological complications: stroke, visual loss, cranial nerve palsy • 0-4% of cases • Causes: plaque disruption v. reflux of particles v. ECAICA anastomotic vessel • Minor complications: facial pain/numbness, trismus, headache, groin hematoma/pain
Discussion • Avoiding neurological complications: • Use of microcatheters that pass into distal branches • Avoiding forceful injection of particles • Identification of dangerous anastomoses – ex: middle meningeal artery • Appropriate particle size
Discussion • Soft tissue necrosis is rare • Likely secondary to extensive collateral blood supply in head and neck • Reports of alar necrosis, nasal septal perforation, oral mucosal and facial sloughing
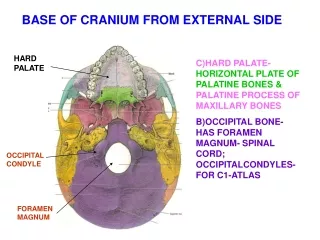
Discussion • Hard palate vascular anatomy: • Major supply from descending palatine artery, branch of IMAX • Anastomoses with sphenopalatine branches at the incisor foramen • Soft palate vasculature provides collaterals: ascending pharyngeal and ascending palatine arteries • Facial artery branches at nasal vestibule supply maxillary gingiva
Discussion • Gauthier, et al (Surg Radiol Anat. 2002): • Performed bilateral descending palatine artery ligations (in setting of Le Fort osteotomies) on cadavers • Subsequent colored latex injection into the carotid artery demonstrated perfusion of the hard palate mucosa via soft palate collaterals (ascending pharyngeal, ascending palatine)
Discussion • In our case, nasopharyngeal balloon may have reduced flow through soft palate collaterals • Bilateral nasal packing may have decreased supply from the nasal cavity via the incisive canal • Presence of packing for two days after embolization may have allowed for sufficient ischemia to cause mucosal necrosis
Conclusions • Hard palate mucosal necrosis is a rare but serious complication of bilateral internal maxillary artery embolization • Early removal of nasopharyngeal and nasal packing may help prevent this complication