Download
1 / 30
330 likes | 888 Views
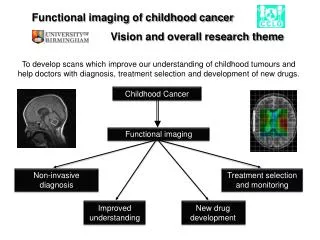
Malnutrition and Nutrition Intervention in Childhood Cancer. Introduction. In United States 10,400 children under 15 diagnosed with cancer in 2007 Overall cure rate for childhood cancer now exceeds 70% Major attention being placed on reducing the side effects of therapy.

E N D
Introduction • In United States 10,400 children under 15 diagnosed with cancer in 2007 • Overall cure rate for childhood cancer now exceeds 70% • Major attention being placed on reducing the side effects of therapy (American Cancer Society 2007)
Introduction • Studies suggest up to 46% of children with cancer experience malnutrition • Malnutrition: characterized by deficiency or excess of energy with measurable adverse effects on clinical outcome • Energy key component of malnutrition, but vitamin & mineral deficiencies also greatly contribute • Children particularly vulnerable (Sala et al 2004)
How To Assess Nutritional Status • No consensus on how to define malnutrition • Most common practices plotting weight-height ratios • Z-scores: more than 2 standard deviations below mean • Other practices include: • Voluntary food intake less than 70% of estimated requirements • Adipose energy reserves (triceps skinfold thickness) less < 5th percentile (Andrassy & Chwals, 1998)
How To Assess Nutritional Status http://www.medscape.org
How To Assess Nutritional Status http://www.ltcconline.net/greenl/courses/201/probdist/zScore.htm
Nutritional Needs of Healthy Children • Normal Children 4-8 years • Calories: 1600 • Protein: 15 grams • Calcium: 800 mg Dietary Reference Intakes (DRIs), AMDR, EER
Nutritional Needs of Children • Children receiving cancer treatment • Increased calorie needs due to raised metabolic rate • Increased protein needs to prevent wasting • 2g/ per kg of body weight per day • Adequate Calcium and Vitamin D intake essential • More than 1,000 mg calcium • More then 10 mg vitamin D • Promote proper bone growth (Shawn and Lawson 2007)
What Causes Malnutrition During Childhood Cancer • One overall common reason – an inability to consume or digest food and nutrients • Side effects of chemotherapy and other aggressive treatments • Increased metabolic demands of the cancer
What Causes Malnutrition During Childhood Cancer Chemotherapy and Aggressive Treatment • Kills rapidly dividing cells, including epithelial cells in digestive tract • Unable to absorb nutrients • Side effects of chemotherapy • Anorexia • Mucositis – inflammation of mucous membranes lining digestive tract • Vomiting • Diarrhea • Alterations in taste • Cachexia: wasting syndrome • Loss of weight and atrophy of muscle, resulting in intense fatigue, weakness (Barr, 2002)
What Causes Malnutrition During Childhood Cancer The Type & Stage of Cancer • The type of cancer also affects nutritional status of child when based on type, stage, and metastatic status of disease (Bauer et al 2011)
What Causes Malnutrition During Childhood Cancer The Type & Stage of Cancer • High Risk Factor for Undernourishment • Advanced Solid Tumors - Neuroblastoma • Aggressive Tumors • Tumors in late stages of malignancy • Moderate Risk Factor for Undernourishment • Nonmetastatic tumors • Diagnosis with favorable prognosis (Bauer et al 2011)
Side Effects of Malnutrition During Cancer • Increased treatment time • Decreased quality of life after survival • Greater chance of becoming underweight or overweight
Side Effects of Malnutrition During Cancer Increased Treatment Time • Malnutrition reduces effectiveness of chemotherapy • Increases length of time children must spend in hospital • Malnutrition also increases likelihood of developing infection (Bauer et al 2011)
Side Effects of Malnutrition During Cancer Decreased Quality of Life After Survival • Lower chances of patients’ survival post-treatment • “Undernourishment has significant role in survival rate especially in children with solid tumors and metastatic diseases…” (Bauer et al 2011)
Side Effects of Malnutrition During Cancer Becoming Underweight or Overweight • Specific cancer types more likely to cause a child to become underweight or overweight later in life if experience malnutrition during treatment (Bauer et al 2011)
Side Effects of Malnutrition During Cancer Becoming Underweight or Overweight Underweight: soft tissue sarcoma, neruoblastoma, non-Hodgkin’s lymphoma, brain tumors, male leukemia patients, non-amputated females with bone cancer, Wilms tumors, survivors of Hodgkin’s disease Overweight: acute lymphoblastic leukemia and those receiving cranial radiation therapy for brain tumors • Possible Reasons total body radiation, abdominal radiation, very young age, use of anthracyclines or actinomycin (Bauer et al 2011)
Side Effects of Malnutrition During Cancer (Bauer et al 2011)
Nutritional Intervention – During Therapy • Supplemental (oral feeding) • Best when patient has reduced oral intake but no change in nutritional status • Be flexible! Studies show flexible menu choice and meal times increase children’s food, protein, and energy intake (Houlston et al., 2009) • Enteral (tube feed) • Best when child’s gut still functioning • Parenteral (intravenously) • Used if child has gut dysfunction >5 days (Houlston et al., 2009)
Comparing The Three Treatments • Past research has indicated when normal oral intake not possible, enteral nutrition has more physiological benefits • Maintenance of height and activity of villi and brush border enzymes • Preservation of specific gut nutrients (glutamine, short-chain fatty acids) • Upholds mucosal membrane • Fewer infections • However many studies are continuing to show parenteral nutrition better at correcting and preventing malnutrition (Braunschweig et al, 2001 and Woodcock et al 2001)
Enteral Compared with Parenteral Nutrition: Meta AnalysisCarol Braunschweig, Paul Levy, Patricia Sheean, Xin Wang • Objective: researchers used results of 27 previous cancer-patients and examined relations among nutrition intervention methods to complications and mortality rates in order to determine whether results supported use of tube feeding instead or parenteral nutrition (Braunschweig et al 2001)
Enteral Compared with Parenteral Nutrition: Meta AnalysisCarol Braunschweig, Paul Levy, Patricia Sheean, Xin Wang • Results: • 27 studies showed lower rate of infection with tube feedings (enteral nutrition) overall • However, when patients already malnourished, parenteral nutrition deemed more effective • Tube-feedings associated with significantly higher risk of mortality and infection (Braunschweig et al. 2001)
Nutritional Interventions – After Therapy • Once children have entered remission, nutrition rehabilitation still may be needed • Chemotherapy side effects may exist such as: • Diarrhea • Constipation • Sore Mouth • Weight Loss/Poor Appetite • Poor Digestion • Combat these ailments nutritionally!
Nutritional Interventions – After Therapy • Study “Dietary Intake after Treatment in Child Cancer Survivors” assessed dietary intake after treatment of childhood cancer survivors • Monitored dietary intake of 50 childhood cancer survivors • Parents kept 3-day food diary (Cohen et al 2011)
Nutritional Interventions – After Therapy • Results: of the 50 Childhood Cancer Survivors • 20% overweight or obese • 54% consuming above their estimated energy requirements • 50% of children did not meet requirements for folate • 32% of children did not meet requirements for calcium • 44% of children did not meet requirements for iron (Cohen et al 2011)
Nutritional Interventions – After Therapy Nutrient Intake of Childhood Cancer Survivors Meeting requirements for all nutrients except: (Cohen et al 2011)
Nutritional Interventions – After Therapy • Conclusion and Implication of Study • Calcium Deficiency: • Greater risk of developing complications related to osteoporosis • Children should consume calcium-rich foods daily (milk, cheese, yogurt) • Participate in weight-bearing exercise (Cohen et al 2011)
Nutritional Interventions – After Therapy Conclusion and Implication of Study Continued • Folate Deficiency: • Link between decreased folic acid and increased risk for homocysteine accumulation • Increase vegetable consumption – especially leafy green vegetables • Fortified foods (fortified cereals, breads, pastas) (Cohen et al 2011)
Nutritional Interventions – After Therapy Conclusion and Implication of Study Continued • Iron Deficiency • Iron deficiency anemia • Red meat • Supplements another alternative • Hard to meet iron requirements (Cohen et al 2011)
Take Home Points • Malnutrition results from chemotherapy and other aggressive treatments & increased metabolic rates due to type of cancer • Main side-effects of malnutrition include: • increased treatment time • decreased quality of life after survival • greater chance of becoming underweight or overweight • Parenteral nutrition best used when child malnourished • After therapy, folate, calcium, and iron most problematic nutrients