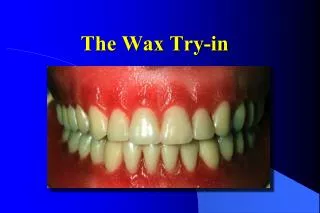

the try-in appointment
E N D
Presentation Transcript
1. The Try-In Appointment Khaled Q Al Hamad
BDS MSc MRD RCSEd
Jordanian Board
Assistant Professor, Faculty of Dentistry
Jordan University Of Science & Technology
3. Denture surfaces
4. Impression: rest on the ridge and transmit forces to the denture bearing areas.
Occlusal: articulating surfaces of the prosthetic teeth that make contact during functuinal and parafunctional movements.
Polished: non articulating parts of the teeth (buccal & lingual) along with the buccal, labial, lingual, and palatal parts of the denture base material
5. Arch form
6. Occlusal Plan
7. Occlusal plan.
8. Landmarks
10. Occlusal relation Occlusal plane
Vertical relation: occlusal vertical dimension.
Antero-posterior /horizontal relation.
11. Occlusal plan.
Incisal .
R & L occlusal planes.
Plane of the mandibular teeth.
12. Verifying the VD Observation of the VD at rest & occlusion.
No precise scientific method.
13. Verifying the RCP Intra-oral observation.
Extra-oral articulator method
Remounting technique.
14. Aesthetic Shape (mould), shade setting(tooth position) compared with age and sex.
Lip support, incisal edge position ( amount of tooth show)
speech ( at a later stage )
15. Speech
16. Posterior palatal extensionPost Dam Identify the hamular notches.
Identify the foveae palatinae.
Locate the vibrating line.
Mark the posterior extension of the denture and trim the denture base accordingly.
Transfer this line to the cast.
draw a line 1mm in front of the first line to indicate the location of the posterior seal.
The bead is 1.5mm in height and width at the base and sharp at the apex.
18. Complete Denture Insertion Khaled Q Al Hamad
BDS MSc MRD RCSEd
Jordanian Board
Assistant Professor, Faculty of Dentistry
Jordan University Of Science & Technology
19. Checks on return from laboratory Rough or sharp points.
Scratch marks indicating poor quality.
Is it too bulky? 3mm ideally.
Is it plaster free ?
Contouring ?
Overpolish of the peripheries? Loss of the peripheral roll?
20. The suggested sequence of events With dentures on the articulated casts, verify that the dentures are in balanced occlusion, and that the incisal pin is in contact with incusal table.
Check working, balancing and protrusive occlusions.
Remove the denture from the cast and ensure that there are no sharp edges or acrylic pearls on the impression surface of the denture.
After infection control, check for overextensions and support.
Confirm the occlusal relationship are acceptable.
Confirm appropriate free way space exists (proper vertical relation).
Let the patient inspect the dentures in a mirror and assess the appearance & speech.
21. Problems with retention ? Overextension of the peripheries.
Underextension of the peripheries
Poor posterior seal of the maxillary denture.
Poor adaptation
Poor stability
Occlusal discrepancies.
22. Checking the Occlusion. The occlusion should be checked in the same way as in the Tri-In appointment and as done on the articulator. First start by verifying the occlusion in RCP. If the laboratory work has been done carefully, the occlusion should be almost perfect. However, due to processing errors, unevenness often occurs, and so the occlusion should be checked Articulating Paper; these are impregnated with different colors of dyes (usually blue on one surface and red on the other) and are produced in different thicknesses. The thinner ones give the most reliable results as they interfere least with the occlusion. Place a piece between the teeth and ask the patient to close in retruded contact position. Remove the denture from the mouth and examine the occlusal surfaces. The occlusal surfaces will exhibit areas of coloration where the cusps and fossae of the opposing teeth have been in contact. These marks should be evenly distributed, but particularly even over the holding cusps( the palatal of the upper and he buccal of the lingual). Areas of hard or uneven pressure will show up as a darker spot. Areas of light contact will show light or no color at all. To equalize the contacts, the fossa opposing the holding cusp is adjusted with a proper bur. The dentures are then whipped to remove the dyes and the process is repeated till an even contact is achieved.
If proper occlusion is not present, a clinical remount is necessary. The procedure involoves the following steps:
Record RCP at an increased Vertical Dimension. The record should not be peroforated. If there is contact, a new record is needed. A suitable recording material includes wax or silicon.
mount the maxillary cast using a facebow transfere( usually needed when the VD is increased but this not supported by research evidence)
Mount the Mandibular casts using the record.
By closing the pin of the articulator, the premature contact will be obvious and can be adjusted.
If the occlusal error is large, the posterior teeth should be removed and waxed added to the base. A new RCP registration should be recorded and tried in wax before processing.
25. Post Insertion Instructions Increase in salivary flow
Start eating with soft food on both side
Sore spots are not unusual and adjustment will be needed
Cleaning Instructions
Clean the dentures after meals by removing and rinsing under tap water. A soft bristle brush and warm soapy water can also be used.
the dentures should be removed at night time( except the first few days to help get used to the new dentures)
Denture cleansers
Alkaline peroxide. The mechanism of action of alkaline peroxide is by producing effervescence that will dislodge foreign materials. They are probably the most damaging to the soft relining materials.
Acid Cleansers. These agents� work by softening the debris. Care should be taken when used with dentures made of metal parts such as Cobalt-Chromium dentures (used commonly in partial dentures) as they can cause corrosion of the metal.
Hypochlorite Cleansers. The mechanism of action for these agents is by bleaching the debris. They appear to cause the least damage to the soft lining materials but may bleach acrylic resin and cause corrosion of metals.
The patient should not use toothpaste or a hard bristles toothbrush, as these will scratch the resin. Furthermore, the dentures should not be soaked in boiling water, as this tend to bleach the dentures.
26. Recall Appointments There is no consensus on this issue, the following schedule is suggesested
Within 3-4 days after the insertion visit.
1 week
1 month
Once the patient is comfortable with the dentures, review appointments could be schedulled on a yearly basis.