1 / 48
480 likes | 494 Views
Basic Fetal Monitoring First of Four with Narration

E N D
Basic Fetal Monitoring Instructor: Kristi Eichhorn BSN, msn, RN-C, WHnp-bc, CNM Nursing Professor - obstetrics AWHONN FHM Instructor Perinatal educator Original BFHM Created By: Eileen Vido BSN, RNC-OB Luann Beacom MSN, MPH, CNS, FNP Karen Harmon MSN, CNS, RNC Ana-Maria Gallo PhD, CNS, RNC
Objectives • By the end of this presentation the participant shall: • Identify the purpose of fetal monitoring • Describe the various methods of monitoring • Understand the physiology and pathophysiology related to the fetal heart rate (FHR) • Identify FHR patterns and related nursing interventions • Have knowledge of antenatal fetal surveillance tests including indications and related nursing interventions
Purpose of FHR Monitoring • To assess the influence of the intrauterine environment for fetal well-being • Identify the fetus at risk • Assess fetal well being • Identify both reassuring and non-reassuring FHR changes • To assess progress of labor through measurement of uterine activity (UA)
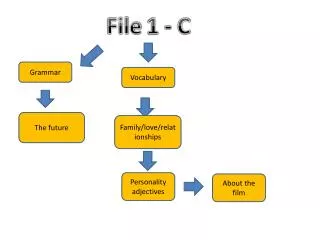
A few examples of what we’ll be discussing… FHR = top squiggly line UA = bottom line Each mountain = uterine contraction
FHR UA
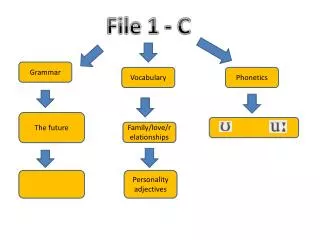
TWINS! FHR Twin B (Bold) FHR Twin A UA
Organization acronyms • AWHONN – Association of Women’s Health, Obstetrics, & Neonatal Nursing • ACOG – American Congress of Obstetrics and Gynecology • ACNM – American College of Nurse-Midwives • NICHD – National Institute of Child Health and Human Development
History of Fetal Monitoring • 1800’s – MDs and Midwives using auscultation via stethoscope • 1960’s – EFM technology developed • 1970’s - Widespread use but inconsistent interpretation & terminology • 1980’s – ACOG: intermittent auscultation equivalent to CEFM when patient is low-risk and 1:1 ratio (still supported today) • 1993 – AWHONN standardized education through EFM courses • 1997 – NICHD published standard definitions of EFM patterns • 2005 – AWHONN & ACOG adopted standardized NICHD terminology • 2008/2009 – standard terminology update and FHM categories added
Methods of Monitoring Fetal monitoring uterine activity monitoring • Auscultation (listening) • Fetoscope or Doppler • Electronic monitoring • External (US) • Internal (FSE) • Palpation only (feeling UC’s) • Electronic Monitoring • External (TOCO) • Internal (IUPC)
Auscultation: Doppler & Fetoscope External Monitoring: U/S & Toco Internal Monitoring: IUPC & FSE
Instrumentation: Electronic Fetal Monitoring • Monitoring equipment • On/Off switch • Test • Display panel • Maternal Vital Sign button • UA Reference • Volume • Mark button
Monitoring Equipment • Graph paper • Monitoring cables • Logic button: • Used for arrythmia recognition • (leave in OFF position)
FHM graph paper/computer screen • Two distinct channels: • Top: Fetal Heart Rate (FHR) • Vertically – records the FHR from 30 to 240 beats per minute • Bottom: Uterine Activity (UA) • Vertically – records the uterine activity from 0 to 100 on a mmHg scale • Measurements of time: • Each small box represents ten (10) seconds of time • Each one of the darkest lines represents 1 minute of time
From darkest line to darkest line = 1 minute Each small box is 10 seconds
From darkest line to darkest line = 1 minute Black and White Image Each small box is 10 seconds. Notice the small boxes have dotted lines.
External Monitor Tocodynamometer “Toco” • Uterine Activity Monitor • Indications for use • Assessment of frequency and duration of contractions • Advantages: • Non-invasive • Can be used for any patient • Membranes do not have to be ruptured
External Monitor Tocodynamometer (cont.) • Disadvantages • Recording UC accurately may be difficult with obesity or preterm labor patients • Location sensitive, improper placement can lead to false information • Unable to accurately detect UC intensity and resting tone • Maternal and fetal motion may be superimposed on waveform • May be uncomfortable • Limits mobility
Artifact Examples on TOCO Tracings: Jagged UA Appearance Maternal pushing efforts during contractions Maternal breathing motions or maternal movement
External Monitor Tocodynamometer (cont.) • Nursing assessment/interventions • Application and placement • TOUCH YOUR PATIENT ! ! ! • Place the toco (button down) on the top of the fundus • Palpate during a contraction to feel where the fundus is firmest • UA reference between UC’s when uterus is soft • Use elastic belt to secure • Patient education • Explain basic element of interpretation, benefits and limitations, and central monitoring
External Monitor Ultrasound Transducer “Doppler” • Contains crystals inside which transmit high frequency US waves and receives reflected waves. • Ultrasounds are motion detectors • Works by detecting cardiac motion • Indications for use • Continuous or intermittent assessment of the FHR
External monitor: ultrasound transducer Advantages Disadvantages Artifact may distort recording Maternal/fetal movement May limit patient mobility Halving and doubling • Non-invasive, membranes may remain intact • Continuous recording possible • Permanent record possible for collaborative decision making and record keeping
180 bpm 180 bpm Example of FHR Halving Pen lifts, small gap in tracing 90 bpm Example of FHR Doubling 140 bpm 70 bpm 70 bpm
External Monitor Ultrasound Transducer (cont.) • Nursing assessment/interventions • Application and placement • Place doppler on the abdomen over area the FHR is heard the strongest • Usually over fetal back • Typically on sides of abdomen, reposition each time patient turns • Secure with elastic belt • Coupling gel must be used because maternal skin reflects ultrasound beams, but the gel allows penetration
External Monitor Ultrasound Transducer (cont.) • Patient Education • Volume • Basic elements of interpretation • E.g., fluctuations of FHR - good • Benefits/Limitations • E.g., may lose signal if baby or mom move • Central monitoring
Internal Monitor Intrauterine Pressure Catheter (IUPC) • Transducer or sensor tipped • Senses intra-amniotic pressure • Indications for use • Accurate assessment & documentation of: • Frequency • Duration • Intensity (in mmHg) of contractions • Uterine resting tone (in mmHg) • Amnioinfusion
www.utahmedical.com Maternity on Pinterest www.pinterest.com Attaches to cable which then plugs into FHM machine
Internal monitor: IUPC Advantages Disadvantages Invasive Potential for uterine or placental perforation Risk for ascending infection Requires ruptured membranes and cervical dilation Requires skill for insertion and calibration Maternal positions affect baseline and contraction intensity • Increased accuracy in all aspects of UA assessment • Increased accuracy correlating FHR to contractions • Accessible port for amnioinfusion • Minimal pressure artifact • E.g., fetal kicks or maternal vomiting • Increased patient comfort (debatable)
Internal Monitor Intrauterine Pressure Catheter (IUPC) • Nursing Assessment/Interventions • Application & Placement • Prepare & set up IUPC per manufacturer guidelines • Observe FHR and maternal status during placement • Once placed, attach IUPC to adapter cable & plug into EFM machine • Zero per manufacturer guidelines
Internal Monitor Intrauterine Pressure Catheter (IUPC) • Nursing Assessment/Interventions • Application & Placement • Sterile Vaginal Exam: determine cervical site and fetal position • Gently displace presenting part, if needed • Use aseptic technique • Insert guide (containing IUPC) between examining fingers • Ensure catheter guide does not extend beyond fingers • Insert up to 45cm or until resistance is met • Attach to cable and confirm device is working
Internal Monitor Intrauterine Pressure Catheter (IUPC) • Nursing Assessment/Interventions • Document: • Maternal/fetal response • Pressure readings (in mmHg, or in Montevideo Units MVU per hospital policy) • Patient Education • Describe purpose & procedure to patient prior to placement • Review benefits/limitations LL, and supine positions
Internal Monitor Fetal Spiral Electrode (FSE) • Measures R to R interval • Indications for use • Continuous fetal monitoring is needed • Ultrasound tracing is incomplete; gaps in tracing • Question of dysrhythmia
Internal monitor: fse Advantages Disadvantages Requires ruptured membranes and cervical dilation Invasive Risk of infection Small risk of fetal hemorrhage Traces any HR May trace maternal HR in presence of demise Missed fetal dysrhythmia if logic button “on” Cannot trace rates > 240 or < 30 bpm) • Continuous tracing and accurate assessment of the fetal heart rate • Fetal arrhythmia recognition • May be more comfortable; belts off abdomen
Internal Monitor Fetal Spiral Electrode (FSE) • Nursing Assessment/Interventions • Application and placement • Cleanse perineum per institutional policy • Pull electrode 1 in. back into introducer so it does not extend beyond the end of the introducer • VE to determine presenting part; feel for firm bone or buttock (Avoid fontanels, sutures, face) • Place introducer between two examining fingers and firmly place against the fetal head at a right angle • Maintain pressure against presenting part & turn clockwise until resistance is met (1-2 times) • Release lock device and remove introducer • Attach monitor to cable device, plug into FHM machine, secure to leg • Document placement and maternal/fetal response
FHR Physiology & Pathophysiology • Fetal Homeostasis • A relationship between fetal heart rate changes, fetal status, fetal oxygenation and fetal acid-base status exists • Can be influenced by maternal, fetal, or placental factors • Fetal Heart Rate • The product of numerous factors that may be loosely divided into: • Fetal intrinsic mechanisms • Maternal-placental extrinsic mechanisms
Fetal Mechanism: ‘Intrinsic Factors’ • Intrinsic Factors: Definition • Fetal mechanisms of FHR control and related fetal cardiovascular anatomy & physiology • Central Nervous System • Autonomic Nervous System • Neurohormonal Factors
From Parer JT: Physiological regulation of fetal heart rate. J ObstetGynecol Neonatal Nurs 5:265, 1976
Medulla Oblongata en.wikipedia.org
Central Nervous System (CNS) BrainSpinal Cord Cerebrum Cerebellum Brainstem Medulla Oblongata Pons Midbrain Reticular formation Peripheral Nervous System (PNS) SomaticAutonomic (primarily voluntary) (involuntary) Sympathetic Parasympathetic (speedy) (pokey) Cranial Nerves Spinal Nerves Adrenal Medulla Nervous System
Central Nervous System • Cerebral Cortex • Causes changes during periods of: • Fetal activity • Fetal sleep • Effected by medication • Medulla Oblongata • Vasomotor centers • Increases or decreases in FHR • Oscillatory changes of FHR variability • Respond to changes in fetal BP, oxygen, CO2 levels, and hormone levels FHR accelerations! Minimal FHR variability