Pulmonary Stenosis
Pulmonary Stenosis. Seoul National University Hospital Department of Thoracic & Cardiovascular Surgery. Pulmonary Stenosis and Intact Ventricular Septum. 1. Definition A form of right ventricular outflow tract obstruction in which

Pulmonary Stenosis
E N D
Presentation Transcript
Pulmonary Stenosis Seoul National University Hospital Department of Thoracic & Cardiovascular Surgery
Pulmonary Stenosis and Intact Ventricular Septum • 1. Definition • A form of right ventricular outflow tract obstruction in which • stenosis is usually valvar or infundibular, or both ( rarely, • supravalvar ) • * Simple, pure, isolated pulmonary valvar stenosis(70%) • * Pulmonary stenosis with normal aortic root • 2. History • Doyen : 1st attempt of surgical relief in 1913 • Sellors : Closed transventricular instrumental valvotomy • repair in 1947 • Brock : Closed valvotomy in 1948 • Swan : Open correction during circulatory arrest in 1952 • Kan : Percutaneous balloon valvuloplasty in 1982
Pulmonary Stenosis and Intact Ventricular Septum • Pathophysiology • Usually involves a stenotic valve that obstructs right ventricular empting and pulmonary blood flow, producing right ventricular hypertrophy and cyanosis. • Subvalvar and supravalvar stenosis are other forms of this defect.
Pulmonary Stenosis and Intact Ventricular Septum • Patterns of pulmonary stenosis 1. Critical valvar pulmonary stenosis • in neonates • 2. Pulmonary stenosis in infants, • children, & adults
1. Pulmonary valve Uniform fibrous cone Pulmonary valve dysplasia 2. Pulmonary arteries Hypoplastic in 50% 3. Right ventricle Mild to moderately reduced Rarely severely reduced Concentric ventricular hypertrophy Diffuse fibrosis 4. Tricuspid valve Normal dimension in 50% Severe hypoplasia in 10% 5. RV-Coronary A. fistulae 2% have fistulae 10% have sinusoids 6. Right atrium Usually large, at least PFO 7. Coexisting cardiac diseases Uncommon Ebstein anomaly in 1% Critical PS in Neonates • Morphology
Clinical Features & Diagnosis • Critical PS in Neonates • 1. Critically ill, irritable, tachypneic, hypoxic • 2. Tachycardia & heart failure, tricuspid insufficiency • may be present • 3. Chest X-Ray, EKG show less evidence • 4. Echocardiography, cardiac catheterization, • cineangiography provide precise information. • 5. Tricuspid valve is competent in 10% & the other • 90% show incompetence.
Critical PS in Neonate • Natural History • 1. Presentation is nearly always within 1st 2 weeks of life. • 2. All neonates in whom severe hypoxia develops die • without treatment, although some may live for a few • months.
Critical PS in Neonate • Operation for Critical PS • 1. Percutaneous balloon valvotomy • 2. Open pulmonary valvotomy using CPB • 3. Transannular patch • 4. Systemic-pulmonary artery shunt • 3.5 - 4.0mm PTFE graft in case of PaO2 • less than 30mmHg after CPB
Critical PS in Neonate • Special features of postoperative care • 1. PGE1 intravenously preoperatively and early • postoperatively to maintain ductal patency • 2. Infants should be restudied at 6-12 months • of age if systemic-pulmonary artery shunt has been • performed . • 3. In about 10% of patients, follow-up evaluation • indicates important residual right ventricular • hypertension.
1. Survival Early death ; less than 10% Time-related survival 2. Modes of death Hypoxia Acute cardiac failure 3. Incremental risk factors for premature death RV enlargement (cardiomyopathy) Reduction of cavity size without shunt 4. Reintervention 5. Residual RVOTO 6. Morphologic & functional changes after valvotomy RV cavity is normal or mildly reduced in 90%. More than 80% of patients ; no tricuspid incompetence Critical PS in Neonate • Surgical Results
Critical PS in Neonate • Indications for operation • 1. Interventional treatment is indicated for all neonates. • 2. Severe hypoplasia of the pulmonary annulus ( z < -4) • & severe reduction of RV cavity size; a transannular • patch & concomitant systemic-pulmonary artery shunt • are indicated in 10-20% of patients as initial procedure. • 3. In patients who fail to develop adequate oxygen level • (more than 85% ) & RA pressure (less than 12-15mmHg) • at rest with atrial septum and shunt temporally closed, • Fontan operation is ultimately indicated.
1. Pulmonary valve Better developed than in neonates Commissural fusion ; deformed, thickened, myxomatous, Secondary infundibular stenosis in older patients 2. Pulmonary artery Poststenotic dilatation in 70% 3. Right ventricle Uncommon hypoplasia Thickening of RV wall 10-20% have only infundibular stenosis 4. Tricuspid valve Usually morphologically normal 5. Right atrium Wall is hypertrophied Patent foramem ovale in most 6. Left ventricle Idiopathic hypertrophic subaortic stenosis (Noonan syndrome) Altered left ventricular geometry affect ventricular function (revert to normal after correction) 7. Associated anomalies Noonan’s syndrome Intrauterine rubella Neurofibromatosis PS in Infants, Children, Adults • Morphology
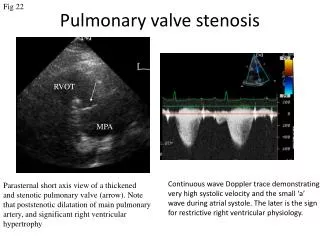
Clinical Features & Diagnosis • PS in Infants, Children, Adults • 1. Symptoms • Symptomatic, but less severe than neonates • 30-40% are asymptomatic. • Effort dyspnea & cyanosis may appear. • 2. Signs • Systolic murmur with a thrill • Pulmonary component of second sound is decreased. • 3. Electrocardiography • RAE, RAD, RVH • T- waves in right precordial lead • 4. Echocardiography, catheterization & cineangiography
Pulmonary Stenosis with IVS • Natural History • 1. Incidence • 8~10% of CHD • Slightly predominance of females • 2. Patients presenting in infancy • Wide variation of obstruction (mild stenosis in 40%, • moderate 47%. Severe 14%) • 3. Patients presenting after infancy • Pressure gradient less than 25mmHg rarely progress. • 4. Effect of right ventricular hypoplasia • 14% of PS have varying degree of hypoplasia & • left untreated, affect unfavorably
Techniques of Operation • PS in Infants, Children, Adults • 1. Comment • Percutaneous balloon valvotomy is treatment of • choice for valvar pulmonary stenosis, if not possible, • open surgical valvotomy is indicated. • 2. Open operation during CPB • Pulmonary valvotomy • Infundibular resection • Transanular patch
Valvar PS ; Operative View( Dysplastic leaflets with commissural fusion )
Special Features & Postoperative Care • PS in Infants, Children, Adults • 1. Withdrawl pressure tracing 24 hrs after operation • 2. Known tendency for infundibular hypertrophy • to regress with time • 3. When the RV is severely hypoplastic, symptoms and • signs are substantially altered, and when they appear • they tend to progress more rapidly. • 4. Pulmonary stenosis with RV hypoplasia is associated • with less than the expected degree of RV hypertrophy. • 5. Balloon valvotomy may not be as effective, & surgical • approach may be required in RV hypoplasia group.
Indications for Operation of PS • PS in Infants, Children, Adults • 1. When patients first show signs & symptoms, at one or • more months of age, pulmonary valvotomy is advisable. • 2. Intervention is advised in asymptomqatic infants with • severe stenosis. • 3. In those with moderate stenosis, intervention is debatable, • when stenosis is mild, not recommended. • 4. In older patients, management differs only in the group • with moderate stenosis. • 5. The presence and degrees of RV hypoplasia are taken • into account when deciding upon intervention.
1. Survival Early deaths ; near zero RV hypoplasia Advanced chronic CHF Time-related survival 2. Complete relief of PS 3. Reoperations 4. Cyanosis When PFO or residual ASD with impaired compliance, & hypoplastic RV 5. Pulmonary incompetence 6. Morphologic changes RV enlarges and becomes normal size in most Tricuspid incompetence is usually absent late postop. 7. Functional Capacity Excellent late result Inferior in hypoplasic ventricle Persistent, recurrent RV failure Surgical Results of PS with IVS • PS in Infants, Children, Adults