Head Injury
Head Injury. Presenters: Abraham Mani Moderator: Prof. D K Pawar. www.anaesthesia.co.in anaesthesia.co.in@gmail.com. Classification of head injury. Mechanism of injury Outcome of the injury. Mechanism of injury . Non- missile or closed head injury . Acceleration – decelaration


Head Injury
E N D
Presentation Transcript
Head Injury Presenters: Abraham Mani Moderator: Prof. D K Pawar www.anaesthesia.co.inanaesthesia.co.in@gmail.com
Classification of head injury • Mechanism of injury • Outcome of the injury
Mechanism of injury Non- missile or closed head injury Acceleration – decelaration Coup - counter coup
Mechanism of injury Missile or penetrating injuries
Brain concussion Transient Reversible Lasting < 6 hours Diffuse axonal injury Deceleration Shearing force LOC > 6 hours (shaken baby synd) Outcome of the injury Diffuse brain injury
Focal brain injury Brain contusion Bruises on the brain
Focal brain injury Epidural hematoma • Blood between skull and • duramater • Arterial bleed • period of lucency • relatively uncommon • present in 1% of all • head-injured patients
Focal brain injury Subdural hematoma > Between the dura mater and the piaarachnoid mater > Occurring in approximately 30% of severe head injuries > It is the underlying brain injury that determines the patient’s course and outcome
Focal brain injury Intracerebral hematoma Impact on the rough surface of the underlying skull base - gliding contusions Can even appear 24 hours following initial insult
Secondary injuries Neuronal damage due to the systemic physiologic responses to the initial injury • Respiratory dysfunction (hypoxemia, hypercapnia). • Cardiovascular instability (hypotension, low cardiac output). • Biochemical substances- excitatory amino acids glutamate and aspartate, cytokines, and free radicals
Pathophysiology of head injury – General overview Head injury Direct tissue damage Impaired autoregulation • Ischemia like pattern • Anaerobic glycolysis • Increased menbrane permeability • Edema • Failure of energy-dependent • membrane ion pumps Exitotoxicity
Pathophysiology of head injury – General overview ischemia excitotoxicity membrane degradation of Vascular and cellular structures necrosis apoptosis
Cerebral blood flow mismatch between CBF and cerebral metabolism Hypoperfusion critical threshold for ischemia -- 15 ml/ 100 g/min CBF The mechanisms : • Morphological injury (e.g. vessel distortion) • Hypotension (autoregulatory failure) • Inadequate availability of nitric oxide or cholinergic neurotransmitters • Prostaglandin-induced vasoconstriction.
Cerebral blood flow Hyperperfusion CBF > 55 ml /100 g/min • Defective autoregulation (vasoparalysis) • increases in cerebral blood volume • increase in ICP
Cerebrovascular autoregulation • Impaired or abolished • Defective autoregulation present immediately after trauma or may develop over time.
CO2-reactivity • CO2-reactivity is intact or even enhanced in most patients • But in severe brain injury CO2-reactivity is impaired
Cerebral vasospasm • Onset varies from post-traumatic day 2 to 15 Mechanisms : • Vascular smooth muscle depolarization • Endothelin • Reduced Nitric oxide • Cyclic GMP depletion • Prostaglandin-induced vasoconstriction • Free radical formation.
Cerebral metabolic dysfunction • Decreased cerebral metabolism (diffuse or focal) • Reduction depends on the severity of primary injury • Decrease or increase of CBF (flow metabolism uncoupling)
Cerebral edema - vasogenic • Mechanical/ autodigestive disruption/ functional breakdown of the endothelial cell layer • Blood-brain barrier disruption • Increases the volume of the extracellular space
Cerebral edema - Ischemia • Increased cell membrane permeability for ions • Ionic pump failure due to energy depletion • Cellular reabsorption of osmotically active solutes Intracellular water accumulation (neurons, astrocytes and microglia)
Inflammatory cytokines and mediators Release of proinflamatory cytokines, prostaglandins, Free radicals and compliment Chemokine and adhesion molecules (ICAM and VCAM) Mobilization of neutrophils
Inflammatory cytokines and mediators neutrophils Adhesion to both defective and intact endothelium Tissue infiltration PG and LT mediated vasoconstriction edema Secondary brain injury
Cardiovascular responses to head trauma • Hypertension • Increased systolic BP and SVR • substantial blood loss hypotension (SBP < 90 mm Hg at admission leads to significantly increased morbidity and mortality)
Respiratory responses to head trauma • Apnea • Abnormal respiratory patterns • Aspiration of vomitus • Central neurogenic pulmonary edema
Neurogenic pulmonary edema • Rapid onset • Relationship to hypothalamic lesions • Massive sympathetic (alpha adrenergic) discharge • Blood shift from systemic to pulmonary circulation • Pulmonary capillary membrane disruption
Temperature regulation • Can be altered • Hyperthermia further brain damage • Hyperthermia should be avoided
Principles of emergency management • First priority is - • Ventilation • Circulation • Stabilize cervical spine • Limited time for initial evaluation of neurological status • Treatment of hemorrhagic shock takes precedence over neurosurgical procedures
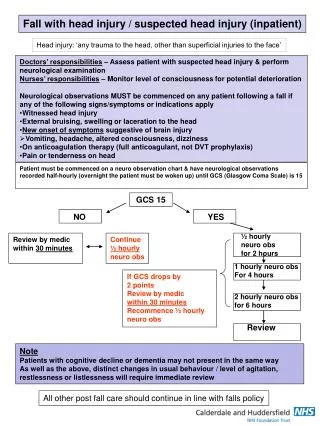
Primary Trauma Survey Stabilize Cx spine, ABC (avoid hypoxia & hypotension) Cx injury present in 6 – 8% Patients with head injury Initial 4 point assessment Alert Responding to voice Responding to pain Unresponsive Assess level of consciousness & Pupil examination
Secondary Trauma Survey • After patient relatively stable • Look for coexisting other organ injuries • Complete neurological examination • Severity of head injury classified by GCS score.
Glasgow coma scale • First described in 1974 by Graham Teasdale and Bryan J. Jennett Lancet 1974, 2:81 • Simplicity • Low inter observer variability • Good predictor of outcome
Affected by : Hypotension Substance abuse Sedation/ paralysis Full assessment of GCS limited by: Periorbital swelling Tracheal intubation Glasgow coma scale
Pupil reactivity Brain stem compromise Poor Reactivity or dilation CN 3 compression Poor reactivity could also be due to hypotension Localizing sign on pupil examination points towards a focal mass lesion
Prognostic significance of GCS and pupil reactivity • Both GCS score (all 3 components) pupil reactivity shows correlation with outcome • Moving target: keeps on changing with time • Post resuscitation assessment shows better agreement Prognostic Value of the Glasgow Coma Scale and Pupil Reactivity in Traumatic Brain Injury Assessed Pre-Hospital and on Enrollment: An IMPACT Analysis . JOURNAL OF NEUROTRAUMA 2007
Tracheal intubation • In patients with GCS < 8 or not able to protect airway • Earliest to avoid hypoxia and secondary brain injury • No sedation or paralysis may be required in these patients • Full stomach - cricoid pressure • Cervical spine injury – Manual in-line stabilization
Airway in head injury patients Opening mouth Jaw thrust Head tilt to be avoided till Cx spine injury is ruled out
Manual in line stabilization To prevent movement of cervical spine
Fluid resuscitation • Fluid resuscitation (based on) • blood pressure • urinary output • central venous pressure (CVP)
To be cont. by Dr. Mani www.anaesthesia.co.inanaesthesia.co.in@gmail.com