Download
1 / 32
360 likes | 2.24k Views
Hayek . M Chest tube related to some indications NSG Collage , Medical complex Najah university. Chest Tubes: Indication to Removal Chest Tube Care and Monitoring.

E N D
Hayek . M Chest tube related to some indications NSG Collage , Medical complex \ Najah university Chest Tubes: Indication to RemovalChest Tube Care and Monitoring
Presenting illness Past medical history Physical assessment: Inspection Palpation Percussion Auscultation of breath sounds and quality of voice Assessment of Respiratory System
Abdominal/Accessory muscles use. Abnormal breath sounds Asymmetrical chest wall motion Decreased oxygen saturation Decreased urine output ECG changes Hyper/hypoventilation Jugular venous distention Nasal flaring Restlessness/confusion/agitation Shortness of breath Skin color changes Tachycardia and hypertension Tracheal shift The Patient in Respiratory Distress
Pneumothorax Hemothorax Symptomatic pleural effusion Empyema Complicated parapneumonic effusion……… ect Indication for Chest Tube Placement
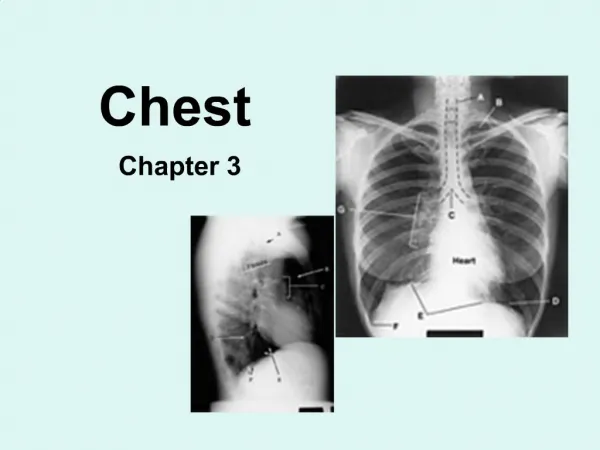
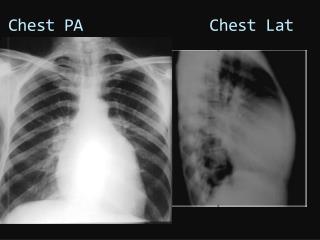
Based on systematic evaluation: Soft tissues of neck, shoulders, breasts, axillae, diaphragms, and upper abdomen Skeletal structures such as clavicles, ribs, vertebrae, scapulae, and sternum Trachea, bronchi, pleural spaces, and lung parenchyma Tubes, lines, and monitoring devices Normal Chest Roentgenogram (X-ray)
Normal Chest X-ray Simple Pneumothorax Comparison of Chest Radiographs(Pneumothorax) Collapsed lung
Collection Bottle: collects fluid and debris delivered by chest tube. Connected to water seal chamber Water Seal Bottle: One way valve for air to escape from the pleural space, measures negative pressure in chest, and determines degree of air leak Suction Control Bottle: Volume of water determines amount of negative pressure in pleural space How Does a Chest Tube Function? Goal is to remove fluid or air from the pleural space, prevent re-accumulation, and allow for lung re-expansion.
Chest Tubes • French sizing refers to the diameter of the tube in millimeters from 8-40 Fr • Tube is sterile, flexible, nonthrombogenic composed of vinyl or silicone • Typically packaged with aluminum trocar • Measures 20 inches in length (50 cm) • Proximal end is fenestrated • Indications and patient size dictates size • Pneumothorax: 20-24 Fr • Fluid: 28 Fr • Average adult/teen male: 28-32 Fr • Average adult/teen female: 28 Fr
Allergic reaction Bronchopleural fistula Cardiac injury Hemorrhage Hepatic injury Infection Intercostal nerve, artery, or vein injury Lung laceration Re-expansion pulmonary edema Splenic injury Subcutaneous emphysema Common Complicationsof Chest Tube Insertion
Conduct routine patient assessment Frequently assess the insertion site, tube, tubing, and drainage unit Monitor amount, color, and consistency of the drainage Encourage positioning with head of bed up to 30 degrees Educate about the benefits of coughing, deep breathing, use of the incentive spirometer, and/or flutter valve every two hours Advocate ambulation and position changes Nursing Responsibilities (care)
Amount, Color, and Consistency • Sudden drainage increases could be indicative of hemorrhage • Changes in drainage from pure liquid to red could indicate hemorrhage • Consistency changes from thin, clear fluid to milky could be evidence of evolving infection • Decreased drainage may be a sign of tube displacement, kinked tubing, or a clot may be obstructing the lumen of the tube
Care of patients with chest tube A . Assess patient for respiratory distress and chest pain, breath sounds over affected lung area, and stable vital signs.B . Observe for increase respiratory distress C . Observe the following: * Chest tube dressing, ensure tubing is patent. * Tubing kinks, dependent loops or clots. * Chest drainage system, which should be upright and below level of tube insertion.
Care of patients with chest tube • D. Provide two shodded hemostats for each chest tube, attached to top of patient’s bed with adhesive tape. Chest tube are only clamped under specific circumstances:* To assess air leak * To quickly empty or change collection bottle or chamber; * To change disposable systems; have new system ready to be connected before clamping tube so that transfer can be rapid and drainage system reestablished * To change a broken water-seal bottle in the event that no sterile solution container is available.
Care of patients with chest tube F. Maintain tube connection between chest and drainage tube intact and taped* Water-seal vent must be without occlusion * Suction-control chamber vent must be without occlusion when suction is used G. Coil excess tubing on mattress next to patient. Secure with rubber band and safety pin or system’s clamp
Care of patients with chest tube H. Adjust tubing to hang in straight line from top of mattress to drainage chamber. If chest tube is draining fluid, indicate time (e.g., 0900) that drainage was begun on drainage bottle’s adhesive tape or on write-on surface of disposable commercial system.* Strip or milk chest tube only per MD/PA orders only * Follow local policy for this procedure * To assess if patient is ready to have chest tube removed (which is done by physician’s order
Care of patients with chest tube • E. Position the patient to permit optimal drainage. • * Semi-Flower’s position to evacuate air (pneumothorax)* High Flower’s position to drain fluid (hemothorax)
Problems solving with chest tube A. Problem: Air leak* Continuous bubbling is seen in water-seal bottle/chamber, indicating that leak is between patient and water seal(a) Locate leak(b) Tighten loose connection between patient and water seal(c) Loose connections cause air to enter system.(d) Leaks are corrected when constant bubbling stops
Problems solving with chest tube * Problem: Bubbling continues, indicating that air leak has not been corrected (a) Cross-clamp chest tube close to patient’s chest, if bubbling stops, air leak is inside the patient’s thorax or at chest tube insertion site(b) Unclamp tube and notify physician immediately!(c) Reinforce chest dressing • Warning: Leaving chest tube clamped caused a tension pneumothorax and mediastinal shift
Problems solving with chest tube * Problem: Bubbling continues, indicating that leak is not in the patient’s chest or at the insertion site(a) Gradually move clamps down drainage tubing away from patient and toward suction-control chamber, moving one clamp at a time(b) When bubbling stops, leak is in section of tubing or connection distal to the clamp(c) Replace tubing or secure connection and release clamp
Problems solving with chest tube * Problem: Bubbling continues, indicating that leak is not in tubing(a) Leak is in drainage system (b) Change drainage system * Problem: Tension pneumothorax is present(1) Problems: Severe respiratory distress or chest pain(a) Determine that chest tube are not clamped, kinked, or occluded. Locate leak(b) Obstructed chest tube trap air in intrapleural space when air leak originates within patient
Problems solving with chest tube * Problem: Absence of breath sounds on affected side (a) Notify physician immediately * Problems: Hyper resonance on affected side, mediastinal shift to unaffected side, tracheal shift to unaffected side, hypotension or tachycardia(a) Immediately prepare for another chest tube insertion (b) Obtain a flutter (Heimlich) valve or large-guage needle for short-term emergency release or air in intrapleural space(c) Have emergency equipment (oxygen and code cart) near patient
Problems solving with chest tube * Problem: Dependent loops of drainage tubing have trapped fluid(a) Drain tubing contents into drainage bottle(b) Coil excess tubing on mattress and secure in place * Problem: Water seal is disconnected(a) Connect water seal(b) Tape connection( may mistake happens)
Problems solving with chest tube * Problem: Water-seal tube is no longer submerged in sterile fluid(a) Add sterile solution to water-seal bottle until distal tip is 2 cm under surface * Problem: Water-seal bottle is broken(a) Insert distal end of water-seal tube into sterile solution so that tip is 2 cm below surface (b) Set up new water-seal bottle(c) If no sterile solution is available, double clamp chest tube while preparing new bottle
What is it? Bubbling seen in the water seal pressure scale. Usually will have some rise and fall with each breath, but constant bubbling is a clue that there could be a problem in: Chest tube drainage system Poorly positioned chest tube Injury to bronchus/esophagus Continued air leak in the lung Assessing Air Leaks (RE)
To help determine the location of an air leak, the chest tube may be clamped near the chest wall: If the air leak disappears, then the “leak” is coming from the patient (i.e. persistent lung injury) If the air leak continues, the leak is coming from a location distal to the clamp….i.e. hole in chest tube, loose connection, leak in the tubing, faulty pleuravac system, etc… Don’t forget to release the clamp!!! Assessing Air Leaks
. Bad Things Happen to Good People • Chest tube gets dislodged: If you hear air leaking, cover site with three sided dressing. If no air is heard, cover with sterile dressing and notify the physician. • Chest drainage unit breaks: change the unit, assess, and notify physician • In emergent situations, tubing could be placed in sterile water/saline at a depth of 2-4 cm to re-establish the water seal
When indication for insertion is no longer present (i.e. resolution of pneumothorax, hemothorax, etc…) No air leak evident the day before considering chest tube removal Drainage less than 50cc/8 hours or 150cc/day Patient able to tolerate chest drainage system being brought to water seal from suction Chest x-ray shows complete re-expansion of the lung When is it Time to Come Out?
Procedure is explained and appropriate pre-medication is performed Assumes supine position with arm above head on side of tube Chest drainage unit brought to water seal and the dressing is removed deep inspiration or exhalation ,the tube is removed with one steady movement Site is dressed and x-ray obtained 24 hours later Dressing the insertion site & after removing it Discontinuing the Chest Tube
SUMMARY Caring for a patient with a chest tube requires problem solving and knowledge application. Remember, a chest tubeis a catheter inserted through the thorax to remove air and fluids from the pleural space and to reestablish normal intrapleural and intrapulmonic pressures. When caring for and maintaining a patient with a chest tube, it is important to note the patency of chest tube, presence of drainage, presence of fluctuations, patient's vital signs, chest dressing status, type of suction, and level of comfort.
? 1- What are chest tubes used for? 2- Where exactly is a chest placed? 3- How does the three-chamber system work? 4- Can suction be bad for the patient? 5- Can you make care for pt who have chest tube?