ecmo FINAL
extracorporeal membrane oxygenator


ecmo FINAL
E N D
Presentation Transcript
overview Dr ismail ahmed Lecturer of anesthesia and intensive care ,MD Al Azhar university 2020
OUTLINES • INTRODUCTION • HISTORY • PRINCIPLE • CIRCUIT & COMPONENTS • TYPES • INDICATIONS and CONTRAINDICATIONS • ECMO MECHANISM • COMPLICATIONS
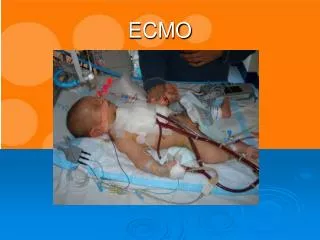
Introduction • EXTRACORPOREAL MEMBRANE OXYGENATION (ECMO) A form of extracorporeal life support(ECLS) where an external artificial circuit carries venous blood from the patient to a gas exchange device (oxygenator) where blood becomes enriched with oxygen and has carbon dioxide removed. The blood is then returned to the patient via a central vein or an artery • ECMO is essentially a modification of the cardiopulmonary bypass circuit which is used routinely in cardiac surgery. • ECMOIt is used as temporary support, usually awaiting recovery of organs SOURCE : ECMO guidelines AlfredHealth Update nov 2015
HISTORY • 1950sDevelopment of membrane oxygenator in laboratory • 1971 First successful case • 1972 First successful paediatric cardiac case • 1975 First neonatal case (Esperanza) • 1975-89 Trial in ARDS, 10% survival • 1990 Standard practice for neonates and pediatrics in some centres • 2000 Standard practice for adults in some centers • 2009 Publication of the CESAR trial which led to a significant growth in the use of ECMO for ARDS cases
ECMO PRINCIPLE • Desaturated blood is drained via a venous cannula ,CO2 is removed, O2 added through an “extracorporeal” device ,then returned to systemic circulation via another vein (VV ECMO) or artery (VA ECMO). • ECMO works by diffusion of gases (O2, CO2) across a semi-permeable membrane • Oxygen diffuses into the blood • Oxygen concentration higher on gas side of membrane , Net diffusion of O2 into the blood
Carbon dioxide diffuses out of the blood flow of the Air-O2 mixture (sweep gas )determines how quickly CO2 is “swept” out of the blood Increase sweep gas flow rate to increase carbon dioxide clearance • Net diffusion of CO2 out of the blood • Titrate flow and fio2 are adjusted to keep PaCO2 pao2 within normal Fick's Law V'gas = D * A * ΔP/T V'gas = Rate of gas diffusion across permeable membrane D = Diffusion coefficient of that particular gas for that membrane A = Surface Area of the membrane ΔP = Difference in partial pressure of the gas across the membrane T = Thickness of the membrane
ECMO CIRCUIT • basic components of ecmo circuit includes • Cannulas • ARTERIAL CANULA SHORT ,WIRE WOUND,SINGLE OUTLET HOLE • VENOUS CANULA LONGER,MULTIPLE OUTLET HOLES • Tubingsthey are of 2 types : regular and heparin coated • Controller and in line monitors • Controller panel for pressure monitoring and blood gas monitoring • membrane oxygenator • Previously, silicon membrane oxygenators were used which are • being replaced by Hollow fibre PMP(polymethyl pentene) • membrane oxygenators. These are extremely efficient at gas • exchange and demonstrate minimal plasma leakage, • low resistance to blood flow.
Blood pump They are basically of 2types. Roller pump , and centrifugal pump Roller pumps are now being replaced by centrifugal pumps. Very reliable , efficient ,low hemolysis • Heat exchanger In adults, it is usually built within the oxygenator. In pediatric , it is connected separately after the oxygenator in the circuit. It is used for temperature regulation of the extracorporeal blood. • Flowmeter and gas blender
CONFIGURATIONS Most common configurations: • Veno-Venous ECMO (VV-ECMO): Used to support patients with severe respiratory failure Blood is drawn from a central vein, pass through an ECMO machine and then returned back via a central vein • Veno-Arterial ECMO (VA-ECMO): Used to support patients with severe cardiac failure Blood is drawn from a central vein, pass through an ECMO machine and then returned back via a central artery ECMO guidelines AlfredHealth Update nov 2015
ECMO INDICATIONS ELSO GUIDELINES: • Acute severe cardiac failure or respiratory failure with high mortality risk and reversible and non-responsive to optimal conventional therapy. • ECMO is considered at 50% mortality risk ( PaO2/FiO2 < 150 on FiO2 >90% and Murray score 2-3) • ECMOindicated at 80% mortality risk. ( PaO2/FiO2 <100 on FiO2 >90% and Murray score 3-4) ELSO General Guidelines Version 1.3 December 2013
ELSO GUIDELINES FOR ADULT RESPIRATORY FAILURE INCLUSION CRITERIA: 1. In hypoxic resp failure due to any cause (primary or secondary) . 2. CO2 retention on Mechanical Ventilation despite high Pplat (>30cm H2O) 3. Need for intubation in a patient on lung transplant list 4. Immediate respiratory collapse (Pulmonary Embolism, blocked airway) unresponsive to optimal care. • Reversible Respiratory Failure examples: ARDS, Severe Pneumonias ,Severe Acute Asthma , Near Drowning ,Post traumatic Lung Contusion,Bronchiolitis Obliterans ELSO General Guidelines Version 1.3 December 2013
CONTRAINDICATIONS No absolute contraindications to ECLS in respiratory failure. Relative contraindications due to poor outcome are : • Mechanical Ventilation at high settings ( FiO2 >90%, P-plat >30) for 7 days or more. • Major pharmacological immunosuppression • CNS hemorrhage which is recent or expanding • Non recoverable co-morbidity such as major CNS damage or terminal Malignancy • Age : no specific age contraindication but increasing risk with age
ELSO GUIDELINES FOR CARDIAC FAILURE • Cardiogenic shock persists despite volume administration, ionotropes and vasoconstrictors and intra-aortic balloon counter-pulsation. typical causes : -Acute myocardial infarction –Myocarditis -Post cardiotomy shock -Peripartum cardiomyopathy ECMO is a Bridge to Recovery : revascularisation, Myocarditis, Postcardiotomy Transplant :Unrevascularizable acute MI, Chronic heart failure Implantable circulatory support : VAD • Septic shock
Initial Settings and Goals • to initiate ECMO U/S guided cannulae are inserted according to the ECMO configuration • the patient is anticoagulated with I /v heparin 50-100 units/kg • connect to ECMO circuit, the pump started with the flow of 20 ml/kg/min and gradually increased every 5-10 min by 10 ml/kg/min to reach the desired flow. ( 50-80 mL/kg/min) • Sweep gas flow 50-80 mL/kg/min • Fractional inspired oxygen (sweep gas) 0.21 -1 % • Once desired flow achieved, ventilator settings are down to base line.(lung reset) ECMO UPTODATE 2013
To achieve these goals : • Oxygen saturation (return cannula) 100% • Oxygen saturation (drainage cannula) > 65% • Arterial oxygen saturation VA > 95%; VV: 85%-92% • Mixed venous oxygen saturation > 65% • Arterial carbon dioxide tension 35-45 mmHg • pH 7.35-7.45 • Mean arterial pressure 65-95 mmHg • Hematocrit 30%-40%
MAINTENANCE & MONITORING • Continuous venous oximetry , Pressure monitoring (pre pump , pre and post oxygenator ), vital parameters , neurological status, vascular status to be monitored. • continuous infusion of unfractionated heparin, titrated with activated clotting time(ACT)of 180- 210 sec. • Daily CXR • Daily bloods: CBC, RFTs, Electrolytes, LFT s • Clotting: ACT first 24 hours then APTT 6 hourly • Plasma free Hb when clinically indicated. The safe range for this is < 0.1g/L. • Blood cultures as indicated.
WEANING INDICATIONS : • For patients with Respiratory failure, improvements in radiographic appearance, pulmonary compliance and oxy Hb saturation. • With cardiac failure, Return or increasing pulsatility on the arterial pressure waveform correlates with improved left ventricular output. Low doses of vasopressors and inotropes. Blood lactate level low and not increasing. Steps • decrease flow to 2L/min then decrease sweep gas FiO2 to maintain SaO2 >95% • When SaO2 stable on these settings, (Low fresh gas flow rates into the circuit (<2 L/min) • Turn off O2 to oxygenator • 6hr stability then de-cannulation SOURCE : ELSO General Guidelines Version 1.3 December 2013
Rush weaning • Forced to remove ECMO even when higher degree of support is required • Indications: Massive bleeding Severe hemolysis Worsening intracranial bleed Infection related to cannula • Risk of continuing ECMO is more than risk of discontinuing ECMO
Anti coagulantion • Although the ECMO circuit has an anticoagulant lining, • Bolus heparin 50-100 units/kg after successful cannulation • followed by continuous infusion. at 10-15units/kg/hour. • Titrate dose to maintain APTT of 50-60s. • Monitor APTT every 6 hours. • Coagulation management • • Activated Coagulation Time -180 -210 s • • Activated partial thromboplastin time of 50 - 60s • • Prothrombin time of 18-24 s • • An internationalized normal ratio of 1.5- 2.0 • • Platelet count more than 50,000/micro litre.
Complications • Bleeding • Clot formation • Cannulation related • VV ECMO specific complications • VA ECMO specific complications • Neurological complications • Hemolysis
Bleeding • Occurs in 30-40% of patients on ECMO • Due to continuous heparin infusion and ECMO induced coagulopathy • treatment : • decrease heparin infusion • maintaining platelet count >50,000/micro litre • target ACT reduces the risk of bleeding.(180-210) • surgical exploration if major bleeding occurs.
Clot formation: • It is more common with VA ECMO than VV ECMO • sudden change in pressure gradient indicates thrombus formation. • Treatmentchange the oxygenator CANNULATION RELATED • Vessel perforation ,Arterial dissection • Bleeding • Distal ischemia in VA ECMO • Treatment : inserting distal perfusion cannula in femoral artery distal to ECMO cannula
VV ECMO SPECIFIC COMPLICATIONS • RECIRCULATION:Here, reinfused blood is withdrawn through the drainage cannula without passing through the systemic circulation.. • INTERVENTION : • Increasing the distance between cannulae OR Addition of another drainage cannula ,dual lumen canula VA ECMO SPECIFIC COMPLICATIONS • retrograde blood flow in the ascending aorta in VA ECMO. stasis of blood can occur if left ventricular output is not maintained. • TREATMENT : • increase the ECMO flow if no cardiac stunning • switch to VV ECMO if persistent lung failure. • Addition of another drainage cannula
Hemolysis • Common in roller pump • Red or dark brown urine • High K+, Renal failure • Jaundice (late sign) Management • Plasma free hemoglobin monitoring • Increase volume • Ultra filtration
ECMO technical advances • Move from roller to centrifugal pumps that do not damage the red cells • Switch from silicone membrane oxygenators to polymethylpentene hollow fibre ones • New Cannula(DUAL LUMEN CANNULA) • Coated “stealth” tubings (nano particles). • Smaller or portable ECMO machines • run with much less Heparin, thus reducing bleeding risk